Dr Richard Hunt
Medical Microbiology and Immunology 650/720

VIROLOGY - LECTURE ELEVEN
HERPES VIRUSES
|
Mercutio (to Romeo) in Romeo and Juliet by Shakespeare: O'er ladies lips, who straight on kisses
dream, |
|
For the complete text of this speech, go here |
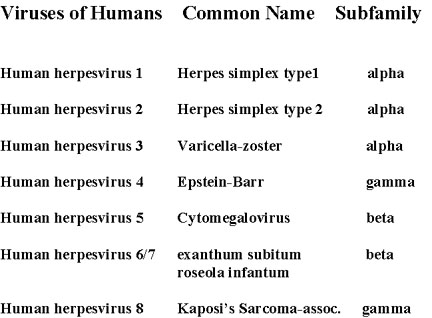 FIGURE 1 Classification of Herpes viruses
FIGURE 1 Classification of Herpes virusesIntroduction
Herpes viruses are a leading cause of human viral disease, second only to
influenza and cold viruses. They are capable of causing overt disease or
remaining silent for many years only to be reactivated, for example as shingles.
The name herpes means comes from the Latin herpes which, in turn, comes
from the Greek word herpein which means to creep. This reflects the
creeping or spreading nature of the skin lesions caused by many herpes virus
types.
There are 25 families in the Herpetoviridae but only six of them are known to infect man with any regularity (table 1 and 2, figure 1)
 Herpes Virus structure. Between the nucleocapsid and the membrane is the
ill-defined tegument
Herpes Virus structure. Between the nucleocapsid and the membrane is the
ill-defined tegument
 Herpes Simplex Virus-1 A-capsid from 400kV Spot-scan Electron Cryomicroscopy
© 1994 Zhou et al. Baylor College of Medicine
Herpes Simplex Virus-1 A-capsid from 400kV Spot-scan Electron Cryomicroscopy
© 1994 Zhou et al. Baylor College of Medicine
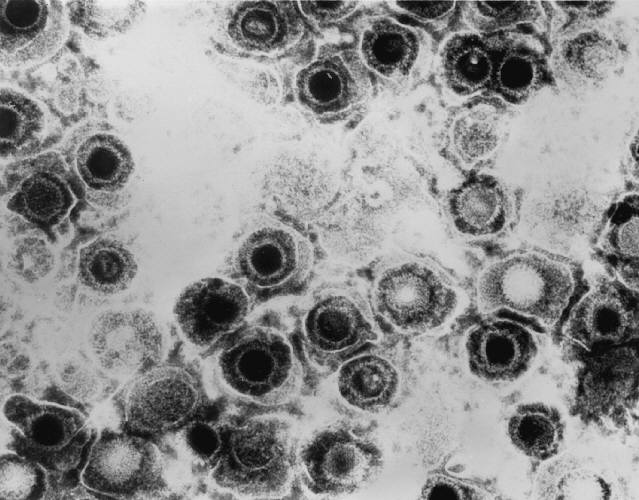
 Herpes simplex virus. Negative stain. Copyright Dr Linda M Stannard, University of Cape Town, South Africa, 1995 (used with
permsssion)
Herpes simplex virus. Negative stain. Copyright Dr Linda M Stannard, University of Cape Town, South Africa, 1995 (used with
permsssion)
|
TABLE 1 HERPES VIRUS TYPES THAT INFECT HUMANS |
| Herpes simplex virus Type 1 (HSV-1) |
| Herpes simplex virus Type 2 (HSV-2) |
| Epstein Barr virus (EBV) |
| Cytomegalovirus (CMV) |
| Varicella Zoster Virus (VZV) |
| Human herpes virus 6 (exanthum subitum or roseola infantum) |
| Human herpes virus 8 (Kaposi's sarcoma-associate herpes virus) |
Once a patient has become infected by herpes virus, the infection remains for life. The initial infection may be followed by latency with subsequent reactivation. Herpes viruses infect most of the human population and persons living past middle age usually have antibodies to most of the above herpes viruses with the exception of HHV-8.
Herpes viruses are classified by their location in the latent state (table 2).
 Liquid-Crystalline, Phage-like
Packing of Encapsidated DNA in Herpes Simplex Virus
(F.P.Booy,
W.W.Newcomb, B.L.Trus, J.C.Brown, T.S.Baker, and A.C.Steven, in CELL, Vol 64 pp 1007-1015, March 8, 1991)
Liquid-Crystalline, Phage-like
Packing of Encapsidated DNA in Herpes Simplex Virus
(F.P.Booy,
W.W.Newcomb, B.L.Trus, J.C.Brown, T.S.Baker, and A.C.Steven, in CELL, Vol 64 pp 1007-1015, March 8, 1991)
 3-D computer reconstruction from cryo-electron micrographs of herpes simplex virus
capsids. Rotating image. National Institutes of
Health
3-D computer reconstruction from cryo-electron micrographs of herpes simplex virus
capsids. Rotating image. National Institutes of
Health
Herpesvirus (entire particle) solved by cryo-electron microscopy and image reconstruction
MPEG version
 Herpesviruses have an envelope surrounding an icosahedral capsid, approximately 100nm in diameter, which contains the dsDNA genome.
When the envelope breaks and collapses away from the capsid, negatively stained virions have a typical "fried-egg" appearance.
Copyright Dr Linda M Stannard, University of Cape Town, South Africa, 1995 (used with
permission)
Herpesviruses have an envelope surrounding an icosahedral capsid, approximately 100nm in diameter, which contains the dsDNA genome.
When the envelope breaks and collapses away from the capsid, negatively stained virions have a typical "fried-egg" appearance.
Copyright Dr Linda M Stannard, University of Cape Town, South Africa, 1995 (used with
permission)
|
TABLE 2 - Properties of Herpes viruses |
|||||
| Human herpes type | Name | Sub Family | Target cell type | Latency | Transmission |
| 1 | Herpes simplex-1 (HSV-1) | Alphaherpesvirinae | Mucoepithelia | Neuron | Close contact |
| 2 | Herpes simplex-2 (HSV-2) | Alphaherpesvirinae | Mucoepithelia | Neuron | Close contact usually sexual |
| 3 | Varicella Zoster virus (VSV) | Alphaherpesvirinae | Mucoepithelia | Neuron | Contact or respiratory route |
| 4 | Epstein-Barr Virus (EBV) | Gammaherpesvirinae | B lymphocyte, epithelia | B lymphocytes | Saliva |
| 5 | Cytomegalovirus (CMV) | Betaherpesvirinae | Epithelia, monocytes, lymphocytes | Monocytes, lymphocytes and possibly others | Contact, blood transfusions, transplantation, congenital |
| 6 | Herpes lymphotropic virus | Betaherpesvirinae | T lymphocytes and others | T lymphocytes and others | Contact, respiratory route |
| 7 | Human herpes virus-7 (HHV-7) | Betaherpesvirinae | T lymphocytes and others | T lymphocytes and others | Unknown |
| 8 | Human herpes
virus-8 (HHV-8)
Kaposi's sarcoma- associated herpes virus (KSHV) |
Gammaherpesvirinae | Endothelial cells | Unknown | Exchange of body fluids? |
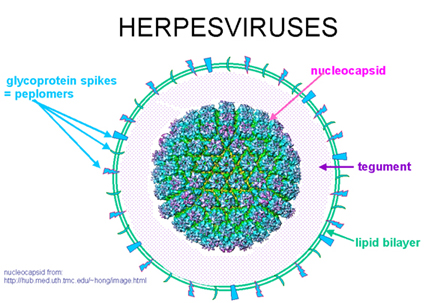
 Glycoprotein "spikes" on the HSV surface. Glycoprotein B (gB) is clearly visualised in clusters of spikes
about 10 nm in length. Between the capsid and the envelope is an ill-defined layer of proteins, collectively known as the tegument.
Copyright Dr Linda M Stannard, University of Cape Town, South Africa, 1995 (used with
permission)
Glycoprotein "spikes" on the HSV surface. Glycoprotein B (gB) is clearly visualised in clusters of spikes
about 10 nm in length. Between the capsid and the envelope is an ill-defined layer of proteins, collectively known as the tegument.
Copyright Dr Linda M Stannard, University of Cape Town, South Africa, 1995 (used with
permission)
FIGURE 2 - Herpes virus structure
Herpes Virus Structure - General
Envelope
Herpes viruses are enveloped viruses. They bud from the inner nuclear
membrane which has been modified by the insertion of herpes glycoproteins (in
the mature virus, these glycoproteins determine the cell to be infected because
of the availability of the appropriate receptors). The viral membrane is quite
fragile and a virus with a damaged envelope is not infectious (This means that
the virus readily falls apart and so the virus can only be obtained by direct
contact with mucosal surfaces or secretions of an infected person - it cannot be
caught from toilet seats). Besides drying, the virus is also sensitive to acids,
detergents and organic solvents as might be expected for an virus with a lipid
envelope.
Tegument
The space between the envelope and the capsid is the tegument. This contains
virally-encoded proteins and enzymes involved in the initiation of replication
Capsid
These viruses have a doughnut shaped capsomere of about 100-200 nm in diameter
with an icosahedral nucleocapsid. The latter contains 162 capsomeres
Genome
These viruses have double stranded DNA. The size of the genomes differs with
cytomegalovirus having the largest genome
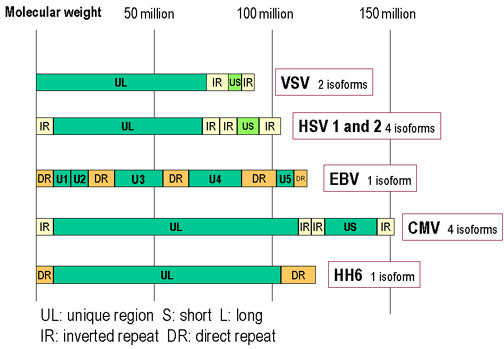 Genomes of herpes viruses. HSV, VZV and CMV have inverted repeat
sequences. This results in the formation of more than one isomer by
recombination. Because VZV has only two inverted repeats, it can only
form two isomeric forms. Direct repeats do not allow recombination and
so EBV and HHV6 have only one isoform.
Genomes of herpes viruses. HSV, VZV and CMV have inverted repeat
sequences. This results in the formation of more than one isomer by
recombination. Because VZV has only two inverted repeats, it can only
form two isomeric forms. Direct repeats do not allow recombination and
so EBV and HHV6 have only one isoform.
FIGURE 3 - Genomes of herpes viruses
i) Binding to the cell surface: As with many other viruses, cell tropism is
determined by the availability of the correct receptor on the surface of the
cell to be infected. The virus fuses with the cell membrane at ambient pH and so
there is the possibility of syncytia formation between infected cells and
therefore cell to cell transmission even in the presence of neutralizing humoral
antibodies. This means that cell-mediated immunity is important in suppressing
herpes virus infections.
ii) Nucleocapsid enters cytoplasm: The tegument-surrounded nucleocapsid is
carried to the nuclear membrane where the nucleocapsid binds. The DNA genome
then enters the nucleus.
iii) Transcription: This is a very complex process, as might be expected from
the large size of genome. There are three classes of proteins that need to be
made for the production of a mature virus.
Alpha proteins: These are the immediate-early proteins. They are involved in transcriptional regulation and are not found in the mature virion. They are also involved in the control of beta protein synthesis (figure 4).
WEB RESOURCES
Movie:
Replication of herpes
(requires Flash)
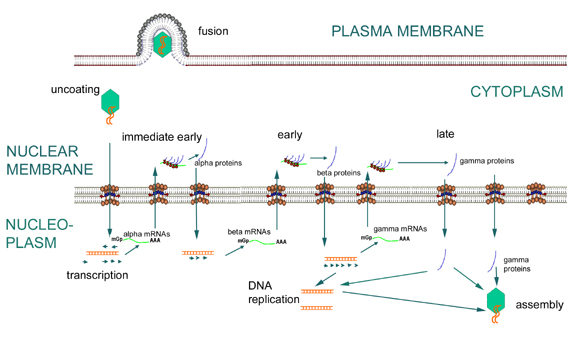 Expression of immediate early, early and late genes of herpesviruses
Expression of immediate early, early and late genes of herpesviruses
FIGURE 4 - Herpes virus gene expression
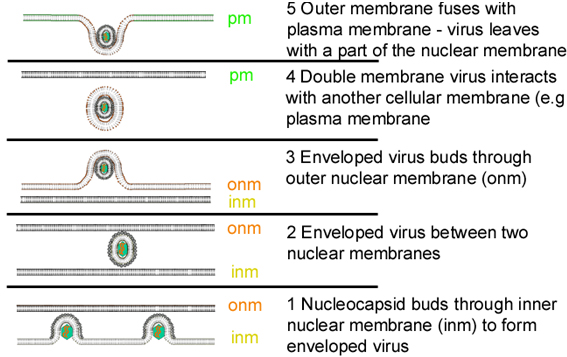 Stages in the exocytosis of herpes virus from the nucleus, in which the virus core is assembled, to the plasma membrane
Stages in the exocytosis of herpes virus from the nucleus, in which the virus core is assembled, to the plasma membrane
FIGURE 5 - Maturation of herpes viruses
Beta proteins. These are the early proteins and are involved also in DNA replication (they include the DNA polymerase and transcription factors). Only a few copies of DNA polymerase need to be made for replication to occur (figure 4).
Gamma proteins. These are the late proteins and are structural components of the virus. The synthesis of gamma proteins is initiated after the start of DNA synthesis (figure 4).
iv) RNA transcription: The herpes DNA is transcribed to RNA by a cellular enzyme (DNA-dependent RNA polymerase I). However, the transcription of the various genes is dependent on both nuclear factors of the cell AND proteins encoded by the virus. This control of viral mRNA, and therefore, viral protein, synthesis determines whether infection will result in the production of new virus particles and cell death (a lytic infection), persistent shedding of virus (persistent infection) or latency. Whether latency occurs is the property of the host cell, that is some cells do not allow the replication of viral DNA. If the cell permits progression beyond the immediate early genes, a lytic infection will ensue.
v) DNA synthesis: Herpes viruses encode their own DNA-dependent DNA polymerase. In addition, some herpes viruses encode enzymes (such as thymidine kinase) that allow the virus to grow in non-dividing cells that do not therefore contain the precursors of DNA synthesis. Without this enzyme, neurotropic herpes viruses could not replicate because of the low amounts of certain DNA precursors in nerve cells.
vi) Assembly: Nucleocapsids are assembled in the nucleus and are filled with DNA They then bud through the double nuclear membrane and leave the cell via the exocytosis pathway or they may bud through another cell membrane such as the plasma membrane (figure 5).
WEB RESOURCES
Animations of Herpesvirus Capsids
Schematic representation of herpes simplex virus infection - animated
Requires Flash
Schematic representation of genes/proteins involved in herpes simplex virus infection - animated
Requires Flash
These are very large viruses and their genome encodes at least 80 proteins. Many of these proteins (about half) are not directly involved in the virus structure or controlling its replication but function in the interaction with the host cell or the immune response of the host.
There are two types, HSV-1 and HSV-2 with very similar characteristics
The genome of HSV also encodes a number of enzymes:
DNA-dependent DNA polymerase
thymidine kinase (phosphorylates thymidine and other nucleosides)
ribonucleotide reductase (converts ribonucleotides to deoxyribonucleotide
serine-protease (convert a scaffolding protein to its final form) (figure 7)
The genome encodes 11 surface glycoproteins. These are involved in:
Attachment (gB, gC, gD and gH)
Fusion of the viral membrane with that of the host cell (gB)
Immune escape and other functions (gC, gE and gI). An example of the immune escape function is gC which binds complement C3 protein and thus depletes it from the host=s serum and inhibits complement-mediated reactions. The virus gE and gI proteins can also bind IgG via the Fc portion of the immunoglobulin. This coats the virus with immunoglobulin and hides it from the immune system.
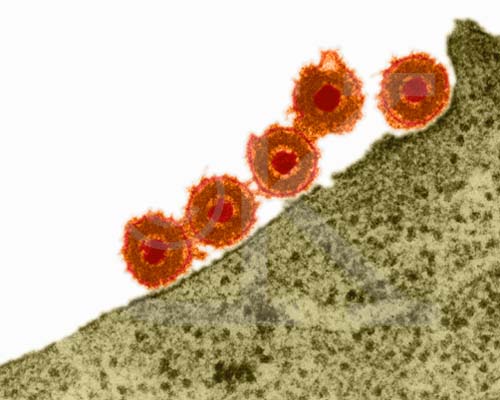 Herpes Simplex Virus (TEM
Herpes Simplex Virus (TEMx169,920) Copyright Dr Dennis Kunkel (used with permission)
 Transmission electron micrograph of herpes simplex virus. Some nucleocapsids are empty, as shown by penetration of electron-dense stain.
CDC/Dr. Erskine Palmer
Transmission electron micrograph of herpes simplex virus. Some nucleocapsids are empty, as shown by penetration of electron-dense stain.
CDC/Dr. Erskine Palmer
FIGURE 6 Herpes simplex virus - Electron micrographs
 The serine protease of herpes viruses. Click on the image at left to
link to an interactive structure of the cytomegalovirus protease. This
protease is essential for the production of mature infectious virions, as it performs proteolytic processing
of a viral assembly protein precursor. (Requires a
Chime plug-in. Get Chime here)
The serine protease of herpes viruses. Click on the image at left to
link to an interactive structure of the cytomegalovirus protease. This
protease is essential for the production of mature infectious virions, as it performs proteolytic processing
of a viral assembly protein precursor. (Requires a
Chime plug-in. Get Chime here)
Figure 7
HSV replication
Almost any human cell type can be infected by HSV. In many cells, such as endothelial cells and fibroblasts, infection is lytic but neurones normally support a latent infection.
Binding
The initial step of the interaction of virus with the cell is binding to the
proteoglycan, heparan sulfate. This molecule is found on the surfaces of many
cells.
Fusion
After binding, the virus fuses directly with the plasma membrane (no entry
into low pH endosomes/lysosomes is necessary). After fusion occurs, the virus
releases some proteins into the cytoplasm. These include some toxins, a protein
kinase and a gene transcription initiator.
Protein synthesis
Immediate early genes are first transcribed which promote transcription of
early genes. If the infection is to be latent, the only mRNAs that are made are
the latency-associated transcripts. The early gene products include the DNA
polymerase plus enzymes that degrade cellular mRNA and proteins. If early and
late proteins are made, the cell is set on a route to lysis.
As noted above, only a few DNA polymerase proteins need to be made for replication of viral DNA. At first, circular concatomers are made but then synthesis switches to linear chains of individual molecules that are cleaved into monomers. This occurs by a rolling circle mechanism (see lecture). Late genes are now transcribed in large amounts, probably triggered by the synthesis of DNA. They are translated in the cytoplasm and transported back into the nucleus where they are assembled into the procapsid. The latter is filled with viral DNA.
Glycoprotein synthesis
All glycoproteins are made in the rough endoplasmic reticulum where they
receive high mannose sugar chains. The glycoproteins are moved to the nuclear
membrane, probably by a process of diffusion since the membrane of the
endoplasmic reticulum is continuous with the outer nuclear membrane. How the
proteins get around the nuclear pore is unknown. The nucleocapsids now bud
through the nuclear membrane via areas in which the viral proteins are
concentrated. In some way, the virus enters the exocytotic pathway since it is
modified in the Golgi body where is receives sugar chains that are
characteristic of Golgi-processed proteins (that is, they contain galactose and
sialic acid).
Release of virus
Several pathways seem to occur. The virus can proceed along the exocytotic
pathway or it can enter the cytoplasm and be released by cell lysis. It also
appears to be able to pass through intercellular junctions and thereby spread
from cell to cell.
Pathogenesis
The hallmark of herpes infection is the ability to infect epithelial mucosal cells or lymphocytes. The virus then travels up peripheral nerves to a nucleated neurone where it may stay for years followed by reactivation. A reddened area gives rise to a macula which crusts to form a papula. The fluid in this blister is full of virus. As long as the virus is kept moist it can remain infectious
Herpes simplex 1 and 2 can infect both humans and other animals but only humans show symptoms of disease. As noted above, HSV-1 and HSV-2 first infect cells of the mucoepithelia or enter through wounds. They then frequently set up latent infections in neuronal cells. The site of the initial infection depends on the way in which the patient acquires the virus. It is often noted that HSV-1 causes infections above the waist and HSV-2 below the waist but this reflects the mode of transmission rather than any intrinsic property of the virus. Both types of HSV can also persistently infect macrophages and lymphocytes. The presence of the virus is often indicated by the formation of syncytia and Cowdry type A inclusion bodies in the nucleus. Once epithelial cells are infected, there is replication of the virus around the lesion and entry into the innervating neurone. The virus travels along the neurone (by a process called retrograde transport) to the ganglion. In the case of herpes infections of the oral mucosa, the virus goes to the trigeminal ganglia whereas infections of the genital mucosa lead the virus entering the sacral ganglia. The virus can also travel in the opposite direction to arrive at the mucosa that was initially infected. Vesicles containing infectious virus are formed on the muscosa and the virus spreads. The vesicle heals and there is usually no scar as a result.
The immune response to HSV 1 and 2
As might be expected, both the cellular and humoral arms of the immune
response are involved. Interferon is important in limiting the initial infection
and natural killer cells are also involved at this stage. Cytotoxic T cells and
macrophages form the cellular arm of the response and kill infected cells. The
humoral arm of the response (usually antibodies against surface glycoproteins)
leads to neutralization. As noted above, the virus can escape the immune system
by coating itself with IgG via Fc receptors and complement receptors. The virus
can also spread from one cell to another without entering the extracellular
space and coming in contact with humoral antibodies. This means that
cell-mediated responses are vital in controlling herpes infections. The cell
mediated and inflammatory response lead to some of the disease symptoms. (Immune
response to herpes: Information
Box)
The virus particles can infect neurones and since only immediate early proteins are made, there is no cytopathic effect (although the presence of the virus can be detected by techniques such as immunofluorescence microscopy using antibodies against the immediate early proteins). Breakage of latency can occur in these cells and the virus travels back down the nerve axon. Lesions now occur at the dermatome, that is the area of skin innervated by a single posterior spinal nerve. This means that recurrence of infection (and therefore symptoms) occurs at the same site as the initial infection. There are several agents that seem to trigger recurrence, most of which are stress-related. It also appears that exposure to strong sunlight and perhaps fever can lead to recurrence. These factors may cause some degree of immune suppression that leads to renewal of virus proliferation in the nerve cell. Recurrent infections are usually less pronounced than the primary infection and resolve more rapidly. (Neurolatency hypotheses: Information Box)
 Site at which HSV-1 and HSV-2 cause disease in humans
Site at which HSV-1 and HSV-2 cause disease in humans
Figure 8
 Herpes simplex virus can set up a primary infection in the lips, move to
the trigeminal ganglion where it can remain latent. Virus can
subsequently reactivate, move to the original site of infection and
result in cold sores
Herpes simplex virus can set up a primary infection in the lips, move to
the trigeminal ganglion where it can remain latent. Virus can
subsequently reactivate, move to the original site of infection and
result in cold sores
Epidemiology
HSV 1 and 2 infections are life-long and although latency is soon set up, the infected patient can infect others as a result of recurrence. The virus is found in the lesions on the skin but can also be present in a variety of body fluids including saliva and vaginal secretions. Despite the apparent above the waist/below the waist rule, both types of HSV can infect oral or genital mucosa depending on the regions of contact (figure 8). However, HSV-1 is usually spread mouth to mouth (kissing or the use of utensils contaminated with saliva) or by transfer of infectious virus to the hands after which the virus may enter the body via any wound or through the eyes. A large proportion of the population has evidence of HSV-1 infection as judged by antibodies. As a result of poor hygiene in underdeveloped countries, HSV-1 antibodies are found in more than 90% of children.
HSV-2 is normally spread sexually and is found in the anus, rectum and upper alimentary tract as well as the genital area. In addition, as noted above, an infant can be infected at birth by a genitally-infected mother. The infant can also be infected in utero if the mother=s infection spreads. Because of the infant=s underdeveloped immune system, the resulting infection can be very severe and sometimes lead to death.
Anyone who comes in contact with fluid containing infectious virus is at risk. There is a disease that affects health care workers called herpetic whitlow that results in lesions on the fingers (it can be caused by either type of HSV). As might be expected, HSV-2 infections are more prevalent later in life as the number of sexual contacts increases. Thus, the lowest rates of infection are found in children and the highest rates in prostitutes among whom as many as 80% are infected with HSV-2.
 Herpes simplex lesion of lower lip, second day after onset.
CDC/Dr. Herrmann
Herpes simplex lesion of lower lip, second day after onset.
CDC/Dr. Herrmann
 Herpes simplex 1: Cold sores
©
Bristol Biomedical Image Archive. Used with permission
Herpes simplex 1: Cold sores
©
Bristol Biomedical Image Archive. Used with permission
 Herpetic gingivitis
© Bristol
Biomedical Image Archive. Used with permission
Herpetic gingivitis
© Bristol
Biomedical Image Archive. Used with permission
 Gingivostomatitis looks different from a cold sore, occurs only once and is usually so mild as to go unnoticed.
© Australian Herpes Management Forum
Gingivostomatitis looks different from a cold sore, occurs only once and is usually so mild as to go unnoticed.
© Australian Herpes Management Forum
Figure 9
Diseases caused by Herpes Simplex Viruses
Herpes simplex 1 and 2 are frequently benign but can also cause severe disease. In each case, the initial lesion looks the same. A clear vesicle containing infectious virus with a base of red (erythomatous) lesion at the base of the vesicle. This if often referred to as a Adewdrop on a rose petal@. From this pus-containing (pustular), encrusted lesions and ulcers may develop.
Oral herpes - Cold sores
As already stated, this can be the result of an HSV-1 or an HSV-2 infection.
Because of the association of HSV-2 with sexual transmission, infections in
children are usually the result of HSV-1. In primary herpetic gingivostomatitis
, the typical clear lesions first develop followed by ulcers that have a white
appearance. The infection, often initially on the lips spreads to all parts of
the mouth and pharynx. Reactivation from the trigeminal ganglia can result in
what are known as cold sores. Herpes pharyngitis is often associated with other
viral infections of the upper respiratory tract. The disease is more severe in
immunosuppressed people such as AIDS patients (figure 9)
Herpes keratitis
This is an infection of the eye and is primarily caused by HSV-1. It can be
recurrent and may lead to blindness. It is a leading cause of corneal blindness
in the United States.
WEB RESOURCES
Cold sores
(Australian
Herpes Management Forum)
Cold sores
(CDC)
 Herpetic whitlow on the wrist © Bristol Biomedical
Image Archive. Used with permission
Herpetic whitlow on the wrist © Bristol Biomedical
Image Archive. Used with permission
Figure 10
This disease of persons who come in manual contact with herpes-infected body secretions can be cause by either type of HSV and enters the body via small wounds on the hands or wrists. It can also be caused by transfer of HSV-2 from genitals to the hands (figure 10).
Herpes gladiatorum
This is contracted by wrestlers. It apparently spreads by direct contact
from skin lesions on one wrestler to his/her opponent, and usually appears in
the head and neck region (which are frequently sites of contact in wrestling
holds). Oddly, the lesions are more often on the right side of the body (perhaps
because most wrestlers are right handed). It is also seen in other contact
sports such as rugby where it is known as scrum pox (Herpes Rugbeiorum):.
 Mother with cold sore on lip holding baby with eczema herpeticum
© Bristol Biomedical Image Archive. Used with permission
Mother with cold sore on lip holding baby with eczema herpeticum
© Bristol Biomedical Image Archive. Used with permission
Figure 11
This is found in children with active eczema, preexisting atopic dermatitis, and can spread over the skin at the site of eczema lesions (figure 11). The virus can spread to other organs such as the liver and adrenals. A similar disease may also be caused by vaccinia (eczema vaccinatum).
WEB RESOURCES
Genital herpes FAQ
(Australian Herpes Management Forum)
Genital
Herpes
(CDC)
Management of Genital Herpes Simplex Infection in Pregnancy
(Australian
Herpes Management Forum)
Genital herpes is usually the result of HSV-2 with about 10% of cases being the result of HSV-1. Primary infection is often asymptomatic but many painful lesions can develop on the glans or shaft of the penis in men and on the vulva, vagina, cervix and perianal region of women (figure 12). In both sexes, the urethra can be involved. In women, the infection may be accompanied by vaginal discharge. Genital herpes infections, which involve a transient viremia, can be accompanied by a variety of symptoms including fever, myalgia, glandular inflammation of the groin area (inguinal adenitis). Secondary episodes of genital herpes, which occur as a result of reactivation of virus in the sacral ganglion, are frequently less severe (and last a shorter time) than the first episode. Recurrent episodes seem usually to result from a primary HSV-2 infection. Patients who are about to experience a recurrence usually first experience a prodrome in which there is a burning sensation in the area that is about to erupt. Some patients have only infrequent recurrences but others experience recurrences as often as every 14-21 days. Whether there is an apparent active disease or not, an infected patient remains infectious without overt symptoms. Clearly, these persons are very important in the spread of herpes infection.
HSV proctitis
This is an inflammation of the rectum and the anus (figure 13).
HSV Encephalitis
This is usually the result of an HSV-1 infection and is the most common
sporadic viral encephalitis. HSV encephalitis is a febrile disease and may
result in damage to one of the temporal lobes. As a result there is blood in the
spinal fluid and the patient experiences neurological symptoms such as seizures.
The disease can be fatal but in the US there are fewer than 1000 cases per year.
HSV Meningitis
This is the result of an HSV-2 infection. The symptoms seem to resolve
spontaneously.
 Genital herpes on the penis © Australian Herpes Management Forum
Genital herpes on the penis © Australian Herpes Management Forum
 Genital herpes on the penis © Australian Herpes Management Forum
Genital herpes on the penis © Australian Herpes Management Forum
 Classical primary genital herpes affecting the vulva. This clinical picture is seen in a minority of
cases © Australian Herpes Management Forum
Classical primary genital herpes affecting the vulva. This clinical picture is seen in a minority of
cases © Australian Herpes Management Forum
Figure 12
 Misdiagnosed perianal herpes. This woman also has severe secondary
Misdiagnosed perianal herpes. This woman also has severe secondary
Staphylococcal infection © Australian Herpes Management Forum
Figure 13
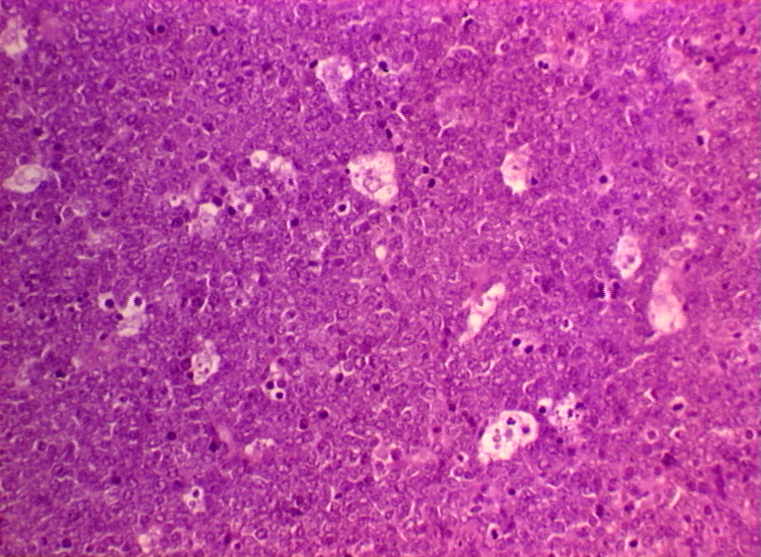
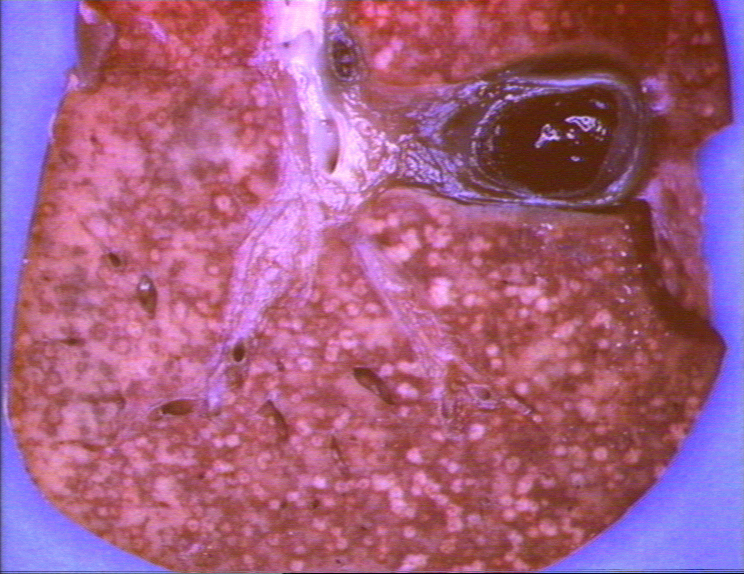 Neonatal herpes simplex infection of the liver © Bristol
Biomedical Image Archive. Used with permission
Neonatal herpes simplex infection of the liver © Bristol
Biomedical Image Archive. Used with permission
Figure 14
This results from HSV-2 and is often fatal, although such infections are rare. Infection is especially possible if the mother is shedding virus at the time of delivery. Thus prospective mothers should avoid contracting herpes during pregnancy. A first episode of HSV-2 infection during pregnancy creates a greater risk of transmission to the newborn. If a woman has active genital herpes at delivery, a cesarean-section delivery is usually performed. The virus can either be obtained in utero or during birth with the latter being more common. Because the neonate has an underdeveloped immune system, the virus can spread rapidly to many peripheral organs (e.g. lungs and liver) and can infect the central nervous system (figure 14).
 Herpes simplex 1, Human Plaque Assay. Cells grown on African green
monkey cells. Phase contrast image. © Bristol
Biomedical Image Archive. Used with permission
Herpes simplex 1, Human Plaque Assay. Cells grown on African green
monkey cells. Phase contrast image. © Bristol
Biomedical Image Archive. Used with permission
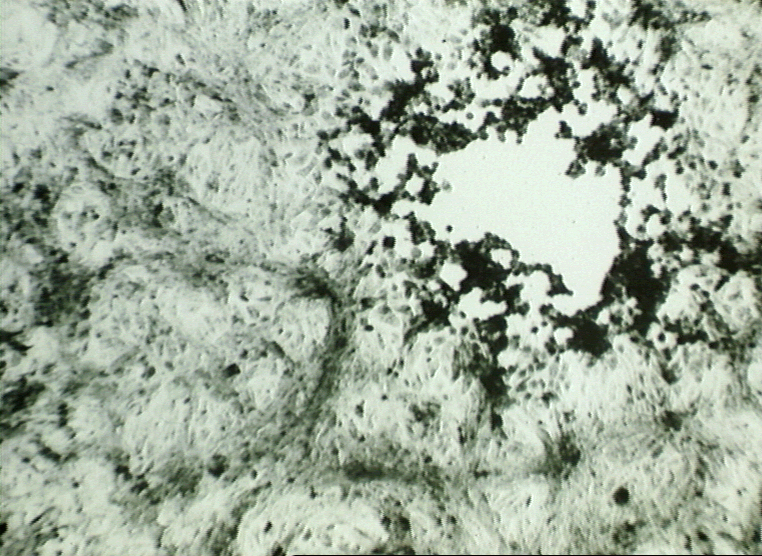
 Herpes simplex 1: Histological stain. Note the multinucleate cell with
dark staining inclusions. ©
Bristol Biomedical Image Archive. Used with permission
Herpes simplex 1: Histological stain. Note the multinucleate cell with
dark staining inclusions. ©
Bristol Biomedical Image Archive. Used with permission
Figure 15
Diagnosis of HSV Infections
Cells may be obtained from the base of the lesion (called a Tzank smear) and histochemistry performed. Since a characteristic of herpes virus is fusion at neutral pH, infected cells can fuse forming syncytia. These can be seen in the smears as multinucleated giant cells and contain Cowdry type A inclusion bodies (figure 15). The cells can also be stained with specific antibodies in an immunofluorescence test and it is also possible to detect viral DNA by in situ hybridization. Type-specific antibodies can distinguish between HSV-1 and HSV-2.
Virus can be isolated from biopsy specimens, that is from the lesions, and grown on tissue culture cells where it forms characteristic cytopathic effects (plaque) including multinucleated cells (figure 15). The presence of anti-HSV antibodies in the patient can be used to form a diagnosis of the primary infection but recurrence is not usually accompanied by a rise in antibody levels.
HSV chemotherapy
There are a variety of nucleoside analog drugs used to treat herpes infections, many of which are of high specificity since they take advantage of the activation of the drug by a viral enzyme, thymidine kinase (see chemotherapy section). The fact that the drug is only activated in herpes-infected cells (because only here is the rather specific viral thymidine kinase expressed) means that these drugs show few side effects.
The best known of the nucleoside analogs is acycloguanosine (acyclovir) but there are other approved drugs including famciclovir and valacyclovir. All of these nucleoside analogs suffer from the appearance of resistant herpes mutants although resistant strains of the virus are usually less virulent than the wild type. It should be noted that these drugs act against the replicating virus (they are incorporated into the DNA as it is copied) and therefore they are ineffective against latent virus.
Since once the virus infects, the patient has it for life, the best option is to avoid infection by not coming in contact with the virus. This is particularly important for health care providers. However, this is not always possible as many patients with active viral replication are asymptomatic. Patients with genital herpes should avoid intercourse when they have the prodromal itching symptoms or an active lesion.
WEB RESOURCES
Varicella-Zoster Virus (also known as Herpes Zoster Virus, Human Herpes Virus-3) (figure 16)
Zoster means girdle from the characteristic rash that forms a belt around the thorax in many patients (figure 18). The structure of Varicella virus is very similar to Herpes Simplex virus although the genome is somewhat smaller
Diseases caused by Varicella-Zoster virus
This virus causes two major diseases, chicken-pox (Varicella), usually in childhood, and shingles, later in life. Shingles (Zoster) is a reactivation of an earlier varicella infection via the cranial nerve.
Chicken Pox
This virus is highly infectious (figure 19) and even if we do not remember getting it, more than 90% of the population of the US has antibodies against varicella proteins. In the household of an infected patient, 90% of contacts who have hitherto not had the disease will get it (unless vaccinated). It is spread by respiratory aerosols or direct contact with skin lesions. As with HSV, infection is via mucosa, this time in the respiratory tract. (Why chicken pox? Information Box)
During the 10-12 day prodromal stage, the virus in the respiratory mucosa infects macrophages and pneumocytes. At this stage, there are no symptoms. The virus spreads from the lungs to lymphocytes and monocytes and to the reticulo-endothelial system. Here, at about 5 days, a second viremia occurs and the virus travels to the skin, mouth, conjunctiva, respiratory tract and, indeed, to epithelial sites throughout the body. Here the virus leaves the blood vessels and first infects sub-epithelial sites and then epithelial sites forming papulae containing multinucleated cells with intracellular inclusions. The virus reaches the surface and is shed to the exterior of the respiratory tract about 12-14 days after the initial infection. It takes a little longer (a few days) for the virus to reach the surface of the skin when the characteristic papulae (rash) appear. At this stage the patient will likely have a fever for a few days (up to 39 degrees). There are various periods between the initial infection and the occurrence of the papulae that are diagnostic of chicken pox but the average is about two weeks with range of 10 to 23 days (figure 17). Spreading of the disease can be from virus in the respiratory tract (by a cough) or from contact with ruptured papulae on the skin containing infectious virus. Thus the contagious period starts at about 12-14 days after the initial infection.
For some reason, the rash is most pronounced on the face, scalp and trunk and less on the limbs. The disease is more severe in older children and adults. This is particularly the case in immunocompromised patients (AIDS, transplantation etc) where the disease may linger for several weeks and the fever may be more pronounced. The spread of the virus may lead to problems in the lungs, liver and to meningitis. In this case mortality may be up to 20%.
Complications
Pneumonia can be associated with a varicella infection (about 15% of adult patients) and may be fatal.
Although most children recover rapidly from the disease, there are some complications. These include fulminant encephalitis and cerebellar ataxia. It is possible that some of these complications may be Reyes syndrome. It has been suggested that the latter may be cause by aspirin used in chicken pox infections. Other rare complications of chicken pox are traverse myelitis, Guillian Barre syndrome and aseptic meningitis.
Congential Varicella syndrome
Major problems may be caused by infection in utero during the first trimester. This is congenital varicella syndrome which leads to scarring of the skin of the limbs, damage to the lens, retina and brain and microphthalmia.
Infection of the mother, who presumably has not previously been infected and therefore does not have anti-varicella antibodies, at around the time of birth can lead to the infection of the infant. Since the infant will not have maternal antibodies against varicella and has immature cell-mediated immunity, it may succumb to the disease with a mortality rate of up to 35%. If the mother becomes infected near to term, both she (before delivery) and her infant (immediately after delivery) should be treated with varicella immune globulin. Most infants, however, get maternal antibodies trans-placentally and are protected from the disease.
 Transmission electron micrograph of varicella- zoster virions from vesicle fluid of patient with chickenpox
CDC/Dr. Erskine Palmer
Transmission electron micrograph of varicella- zoster virions from vesicle fluid of patient with chickenpox
CDC/Dr. Erskine Palmer
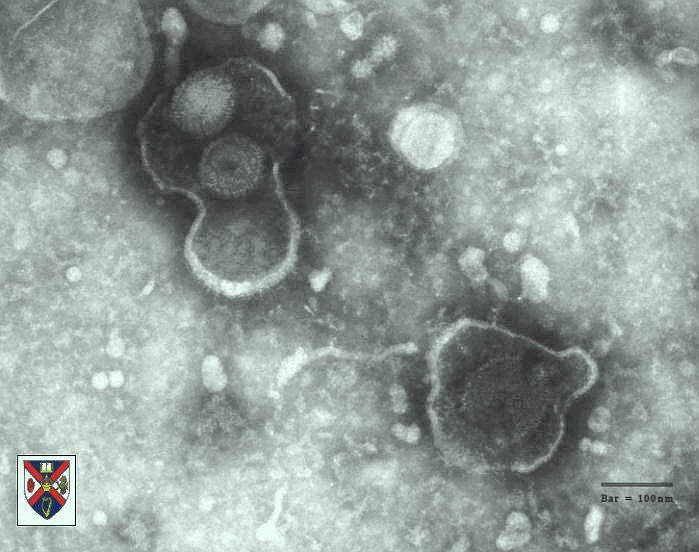 Negative stain of varicella zoster virus © Dr S.
McNulty, Queens University, Belfast. Image must not be used for commercial purpose without the consent of the copyright owners.
Negative stain of varicella zoster virus © Dr S.
McNulty, Queens University, Belfast. Image must not be used for commercial purpose without the consent of the copyright owners.
Figure 16
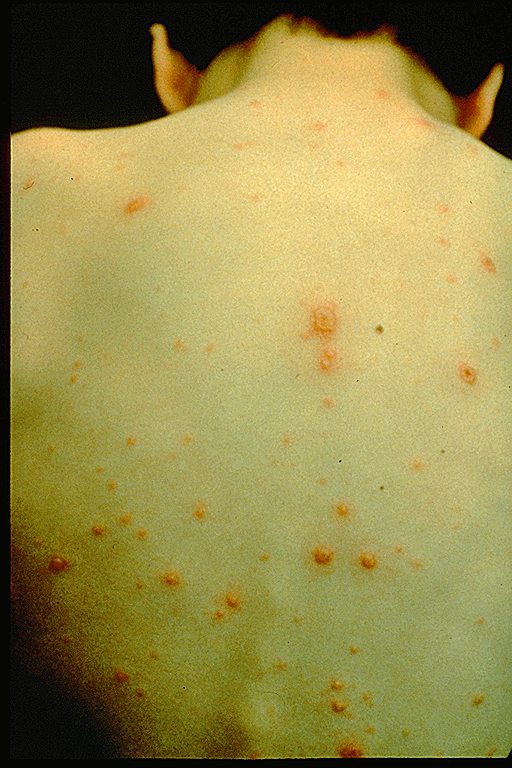
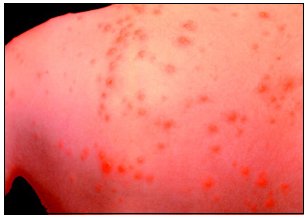 This person has chickenpox rash. Some of the sores are red spots and some are blisters.
The red spots will become blisters and new red spots will form CDC
This person has chickenpox rash. Some of the sores are red spots and some are blisters.
The red spots will become blisters and new red spots will form CDC
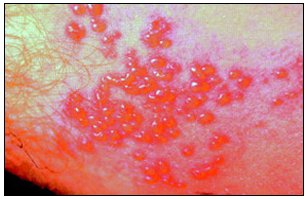
 Each spot starts as a 2-4 mm diameter red papule which develops an irregular outline (rose petal) as a
small vesicle appears on the surface. This 'dew drop on a rose petal' appearance is very characteristic of
chickenpox. © Australian Herpes Management Forum
Each spot starts as a 2-4 mm diameter red papule which develops an irregular outline (rose petal) as a
small vesicle appears on the surface. This 'dew drop on a rose petal' appearance is very characteristic of
chickenpox. © Australian Herpes Management Forum
 This is a classic case of chickenpox of the newborn. The infant contracted
chickenpox at birth from her infected mother.
A severe skin infection has developed on the face and neck and, without treatment, this
infection could spread throughout the
body and cause serious illness or even death
Courtesy of the American Academy of Pediatrics, Pennsylvania
chapter - Immunization Action Coalition
This is a classic case of chickenpox of the newborn. The infant contracted
chickenpox at birth from her infected mother.
A severe skin infection has developed on the face and neck and, without treatment, this
infection could spread throughout the
body and cause serious illness or even death
Courtesy of the American Academy of Pediatrics, Pennsylvania
chapter - Immunization Action Coalition
Figure 17
WEB RESOURCES
CDC
- Shingles
Medinfo
- Shingles
Dematology
Forum - Shingles and Chickenpox
NIAID
Factsheet - Shingles
After the infectious period, the virus may migrate to the ganglia associated with areas in which the virus is actively replicated. The virus may then be reactivated under stress or with immune suppression. This usually occurs later in life. The recurrence of varicella replication is accompanied by severe radicular pain (figure 18) in discrete areas, those innervated by the nerve in which latent infection has occurred. A few days later chicken pox-like lesions (figure 18) occur in restricted areas (dermatome) that are innervated by a single ganglion. New lesions may appear in adjacent dermatomes and even further afield. Reactivation can affect the eye via the trigeminal nerve (uveitis, keratitis, conjunctivitis, ophthalmoplegia, iritis) and the brain via the cranial nerve VII and VIII (Bell's palsy (Bell's Palsy: Information Box) and Ramsay-Hunt syndrome (Ramsay-Hunt: Information Box) (figure 18)). The skin lesions are somewhat different from those in chicken pox, being restricted to small areas of the skin, usually in the thorax (figure 18). They are small and close together. They are maculopapular with an erythematous base and usually heal in about two weeks. Reactivation can lead to chronic burning or itching pain called post-herpetic neuralgia which is seen primarily in the elderly. The pain may last well after the rash has healed (even months or years). Often associated with post-herpetic neuralgia is increased sensitivity to touch (hyperesthesia).
Patients with AIDS often exhibit multi-dermatomal recurrence of varicella infection. There is also a chronic verricous form in some AIDS patients.
 Typical isolated rash in shingles CDC
Typical isolated rash in shingles CDC
 Shingles affecting the left side of the trunk
Shingles affecting the left side of the trunk
 Recurrent varicella zoster on the right side of the face © Bristol
Biomedical Image Archive © Australian Herpes Management Forum
Recurrent varicella zoster on the right side of the face © Bristol
Biomedical Image Archive © Australian Herpes Management Forum
Severe atypical episode of shingles affecting the trunk of a person with impaired immunity. Note that the distrubution of the lesions rersembles a 'sword belt'. Hence the name zoster © Australian Herpes Management Forum
 In severe cases of shingles, the lesions coalesce, forming a disfiguring carpet of scabs and sometimes the rash leaves permanent
scars © Australian Herpes Management Forum
In severe cases of shingles, the lesions coalesce, forming a disfiguring carpet of scabs and sometimes the rash leaves permanent
scars © Australian Herpes Management Forum Disseminated lesions affecting multiple dermatomes © Australian Herpes Management Forum
Disseminated lesions affecting multiple dermatomes © Australian Herpes Management Forum Shingles affecting the right L1 dermatome © Australian Herpes Management Forum
Shingles affecting the right L1 dermatome © Australian Herpes Management Forum Ramsay-Hunt syndrome affecting the ear showing blistering of the
external ear canal © Australian Herpes Management Forum
Ramsay-Hunt syndrome affecting the ear showing blistering of the
external ear canal © Australian Herpes Management Forum Ramsay-Hunt syndrome causing a right-sided facial palsy. Paralysis is more obvious in cases of shingles involving the
face. It is caused by an extension of the disease process to motor regions of the spinal
cord or brainstem. In a minority of cases, the areas of paralysis and rash do not
coincide. For instance, rash on the neck and lower part of the face, involving the
trigeminal and cervical nerves, may be associated with paralysis of the facial nerve and
loss of taste. This distribution of rash and combination of motor and sensory symptoms
cannot be explained by involvement of a single nerve ganglion or a mixed motor and
sensory nerve trunk. Rather, it must be the result of a wider, if still local, spread of virus
in the central nervous system. © Australian Herpes Management Forum
Ramsay-Hunt syndrome causing a right-sided facial palsy. Paralysis is more obvious in cases of shingles involving the
face. It is caused by an extension of the disease process to motor regions of the spinal
cord or brainstem. In a minority of cases, the areas of paralysis and rash do not
coincide. For instance, rash on the neck and lower part of the face, involving the
trigeminal and cervical nerves, may be associated with paralysis of the facial nerve and
loss of taste. This distribution of rash and combination of motor and sensory symptoms
cannot be explained by involvement of a single nerve ganglion or a mixed motor and
sensory nerve trunk. Rather, it must be the result of a wider, if still local, spread of virus
in the central nervous system. © Australian Herpes Management ForumFigure 18 above
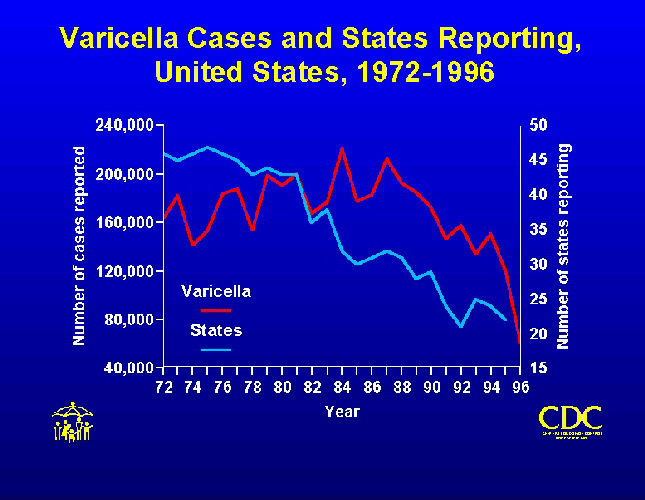 Varicella cases and states reporting, United States, 1972-1996.
CDC/Barbara Rice
ber2@cdc.gov
Varicella cases and states reporting, United States, 1972-1996.
CDC/Barbara Rice
ber2@cdc.gov
Figure 19
Diagnosis
Both chicken pox and shingles are diagnosed by their characteristic appearance but a definitive diagnosis can be made by culture of the virus from the lesions (a difficult procedure) followed by detection of specific antigens. The characteristic appearance of cells in biopsy specimens of skin lesions can also be used.
Treatment
As with HSV, acyclovir (or other nucleoside analogs) can be useful, particular in preventing dissemination in immunosuppressed patients. Varicella immunoglobulin can also be used. Normally, however, only supportive care is used in children who quickly recover if they mount an adequate cell-mediated response.
Vaccine
There is a live attenuated vaccine virus and this is used in the United States. It leads to antibody production and cell-mediated immunity. It can be used post-exposure.
Epstein- Barr Virus
Epstein-Barr virus is the causative agent of Burkitt=s lymphoma in Africa, nasal pharyngeal carcinoma in the orient and infectious mononucleosis in the west. It was first discovered as the causative agent of Burkitt=s lymphoma and it was later found that patients with infectious mononucleosis have antibodies that react with Burkitt=s lymphoma cells.
Receptors for the virus
The virus only infects a small number of cell types that express the receptor for complement C3d component (CR2 or CD21). These are certain epithelial cells (oro- and naso-pharynx) and B lymphocytes. This explains the cellular tropism of the virus.
Semi-permissive replication
B lymphocytes are only semi-permissive for replication of the virus and infection may either be latent or the cells may be stimulated and transformed by the virus. When lymphocytes are latently infected the cell contains a few unintegrated copies (episomes) of the virus genome which are replicated every time the cell divides. In this case the early immediate genes are expressed including the EBV nuclear antigens. In addition, two latent membrane proteins, a protein designated LP (a DNA-binding protein) and two small RNA molecules are expressed. The membrane proteins are oncogenes.
Permissive replication
In contrast, epithelial cells permit complete lytic replication of the virus. Epithelial cells allow the expression of the ZEBRA protein which activates early genes resulting in expression of the polymerase and DNA replication. Subsequently, capsid proteins and the membrane glycoproteins are made.
Pathogenesis
i) Transformation of B cells
The virus is replicated in pharyngeal epithelial cells, shed into the saliva
and is taken up by CD21+ B lymphocytes. These cells are normally short-lived,
dying by apoptosis. This is a natural process that allows cells to be generated
for a particular process and then removed when no longer needed. Although B
cells do not show any histological alterations as a result of EBV infection,
they are stimulated to divide and are protected from undergoing apoptosis; thus,
the cell becomes transformed and high levels of monocytes are seen in the
bloodstream. Transformation of the B cell changes the interaction of the cell
with other components of the immune system. HLA markers, CD23 blast antigen and
certain adhesion proteins are expressed. The presence of the virus results in
the expression of an analog of interleukin-10 (IL-10) which inhibits gamma
interferon secretion. This results in the inhibition of T cell responses and
promotes growth of the B cells and IgG secretion. The virus also causes the
cells to produce other cytokines including IL-5 and IL-6.
ii) Burkitt's lymphoma
The association between Epstein-Barr virus and Burkitt's
lymphoma has long been established. This is a tumor of the jaw and face found
in children (figure 20). The tumor cells show evidence of EBV DNA and tumor antigens and
patients show a much higher level of anti-EBV antibodies than other members of
the population. Tumor cells are monoclonal and show a very characteristic
translocation between chromosomes 8 and 14. This brings the c-myc next to the
gene for the immunoglobulin heavy chain. As a result, the oncogene is next to
the promotor for a gene that is highly expressed in B lymphocytes resulting is
elevated transcription of c-myc. It should be noted that this translocation is
not seen in infectious mononucleosis patients. Biopsy tissue shows large
multinucleated cells (figure 21). Further evidence that
implicates EBV in Burkitt's lymphoma
is the observation that EBV can transform B lymphocytes in culture and can
produce B cell lymphomas in primates.
This lymphoma is endemic in equatorial Africa but only occurs rarely
elsewhere. Why this is so is unclear but there is probably a genetic reason
possibly involving an association with malaria. Persons who are resistant to
malaria appear to be susceptible to progression to the lymphoma.
 Burkitt's Lymphoma The Johns Hopkins Autopsy Resource
(JHAR) Image Archive
Burkitt's Lymphoma The Johns Hopkins Autopsy Resource
(JHAR) Image Archive
Figure 20
 Burkitt;s lymphoma histological stain. Notice the large multinucleated
cells
Burkitt;s lymphoma histological stain. Notice the large multinucleated
cells
© Bristol Biomedical Image Archive. Used with
permission
Figure 21
 Oral hairy leukoplakia of tongue in AIDS
© Bristol
Biomedical Image Archive
Oral hairy leukoplakia of tongue in AIDS
© Bristol
Biomedical Image Archive
Figure 22
iii ) Nasopharyngeal cancer
This disease, which occurs in a number of areas (south China, Alaska,
Tunisia, east Africa), is also associated with EBV. There may be a genetic
predisposition to the development of EBV cancers in these populations or there
may be an environmental cofactor involved. The disease is a tumor of the
epithelium of the upper respiratory tract and the cells contain EBV DNA. The
titer of anti-EBV antibodies alter as the tumor progresses.
iv) Oral hairy leukoplakia
This EBV-associated disease results in lesions in the mouth and has
increased in frequency recently as it is an opportunistic infection of
HIV-infected patients (figure 22).
WEB RESOURCES
The primary infection is often asymptomatic but the patient may shed infectious virus for many years. Some patients develop infectious mononucleosis after 1-2 months of infection. The disease is characterized by malaise, lymphadenopathy, tonsillitis (figure 23), enlarged spleen and liver and fever. The fever may persist for more than a week. There may also be a rash. The severity of disease often depends on age (with younger patients resolving the disease more quickly) and resolution usually occurs in 1 to 4 weeks.
Although infectious mononucleosis is usually benign, there may be complications. These include neurological disorders such as meningitis, encephalitis, myelitis and Guillain-Barrè syndrome. (Guillain-Barrè Syndrome: Information Box) Secondary infections, autoimmune hemolytic anemia, thrombocytopenia, agranulocytosis, aplastic anemia may also occur. As noted above a chronic syndrome may also occur. The symptoms are similar to those reported for chronic fatigue syndrome (headaches, sore throat and low fever) but EBV is probably not the cause of chronic fatigue syndrome.
 Tongue and palate of patient with infectious mononucleosis.
CDC/Emory U./Dr. Sellers
Tongue and palate of patient with infectious mononucleosis.
CDC/Emory U./Dr. Sellers
Figure 23
In infectious mononucleosis, infected B cells are also transformed. The infected B cells proliferate and activate suppressor CD8 T cells. These T cells differ from normal T cells in appearance and are known as Downey cells. The T cells increase in number in the circulation and may account for up to 80% of the white blood cells. This T cell response results in enlarged lymph glands (and enlarged liver and spleen). The activation of the T cells limits the proliferation of B cells and the disease resolves.
If cell mediated immunity is suppressed, resolution of the disease may not occur. Uncontrolled viral replication may lead to a severe syndrome with B cell lymphoproliferation, leukopenia and lymphoma. In patients with T cell deficiency X-linked lymphoproliferative disorder may occur. Transplant patients and AIDS patients who are also immunosuppressed may exhibit post-transplant lymphoproliferative disorder
Epidemiology
A large proportion of the population (90-95%) is infected with Epstein-Barr virus and these people, although usually asymptomatic, will shed the virus from time to time throughout life. The virus is spread by close contact (kissing disease). Infection is associated with socioeconomic factors and in developing countries, seropositivity is observed at an earlier age than in developed countries. Up to 80% of students entering college in the US are seropositive for the virus and many of those that are negative will become positive while at college. The virus can also be spread by blood transfusion.
Diagnosis
In infectious mononucleosis, blood smears show the atypical lymphocytes (Downey cells). There are also serological tests available. Heterophile antibodies are produced by the proliferating B cells and these include an IgM that interacts with Paul-Bunnell antigen on sheep red blood cells.
Treatment
Unlike herpes simplex virus, there are no drugs available to treat Epstein-Barr virus. This may reflect the absence of a thymidine kinase encoded by this virus (drugs such as acyclovir that are active against herpes simplex are activated by the viral thymidine kinase). A vaccine is being developed.
WEB RESOURCES
Cytomegalovirus has the largest genome of all herpes viruses and appears only to replicate in human cells. Its name derives form the fact that, like other herpes viruses, it can form multinucleated cells (syncytia) with characteristically staining inclusions. Some cells such as macrophages and fibroblasts support a productive infection while a latent infection is set up in several cell types including T lymphocytes and stromal cells of the bone marrow. There is only one serotype.
Transmission
Cytomegalovirus infection is found in s significant proportion of the
population. As with Epstein-Barr virus (also spread in saliva), seropositivity
increases with age. By college age, about 15% of the US population is infected
and this rises to about half by 35 years of age. The virus is spread in most
secretions, particularly saliva, urine, vaginal secretions and semen (which
shows the highest titer of any body fluid). Cytomegalovirus infection is
therefore sexually transmitted. It can also spread to a fetus in a pregnant
woman and to the newborn via lactation, though there is some doubt about the
importance of milk transmission. In the hospital, the virus can also be spread
via blood transfusions and transplants. In third world countries with more
crowded conditions, the virus is found in a much higher proportion of the
population than in western countries.
Pathogenesis
Cytomegalovirus causes no symptoms in children and at most mild disease in
adults (but see below). The virus first infects the upper respiratory tract and
then local lymphocytes. Circulating lymphocytes then spread the virus to other
lymphocytes and monocytes in spleen and lymph nodes. The virus finally spreads
to a variety of epithelial cells including those of salivary glands, kidney
tubules, testes, epididymis and cervix. Infection is usually asymptomatic
(sub-clinical) but glandular fever is sometimes seen in young adults. The virus
can inhibit T cell responses. The virus elicits both humoral antibodies and
cell-mediated immunity but the infection is not cleared. Cell-mediated immunity,
not humoral antibodies, controls the infection The importance of cell-mediated
immunity stems from the possibility of spread from cell to cell. Although
suppressed, the virus may later reactivate, particularly in cases of
immunosuppression; indeed, infection by the virus can, itself, be
immunosuppressive.
Congenital disease
There are two instances in which cytomegalovirus can cause serious disease.
During a primary infection of the mother, the virus can spread via the placenta
to the fetus and congenital abnormalities can occur; in fact, this virus is the
most common viral cause of congenital disease. Up to one in forty newborns in
the United States are infected by the virus. Abnormalities include microcephaly,
rash, brain calcification and hepatosplenomegaly. These may result in hearing
loss (bilateral or unilateral) and retardation. As might be expected, when
reactivation occurs in a pregnant mother (usually reactivation in the cervix),
the symptoms are less severe because of the mothers seropositivity. In this
case, congenital abnormalities are rare.
Besides infection in utero, infants may be infected perinatally. As noted above, one tissue in which cytomegalovirus can set up a latent infection is the cervical epithelium and immunosuppression associated with pregnancy can lead to reactivation. About 50% of children born to such mothers are infected and can themselves shed virus within a few weeks. Also breast epithelium can harbor latent virus that may be similarly reactivated leading to infection of the infant. In neither case is there usually a problem and the infant remains asymptomatic.
Neonates may also receive the virus through infected blood transfusions. In this case, the amount of virus is much higher and symptoms may occur. These usually consist of pneumonia and hepatitis.
Disease in immunosuppressed patients
In patients who have received an organ transplant or have an
immunosuppressive disease (e.g. AIDS), cytomegalovirus can be a major problem.
Particularly important is cytomegalovirus-retinitis in the eye which occurs in
up to 15% of all AIDS patients. In addition, interstitial pneumonia, colitis,
esophagitis and encephalitis are seen in some patients.
Diagnosis
Most infections are asymptomatic and therefore go undiagnosed. There are
fluorescent antibody and ELIZA tests. Multinucleated (cytomegalinic) cells with
characteristic inclusions can be seen in biopsies of many tissues.
Treatment
Ganciclovir, which inhibits the replication of all human herpes viruses, is
usually used, especially to treat retinitis. Foscarnet is also approved in the
US. Acyclovir is not effective. A vaccine is being developed but the best way to
avoid the virus is to restrict contact between infected children and pregnant
women. Also since cytomegalovirus is sexually transmitted, condoms can limit
spread.
OTHER HERPES VIRUSES
This virus is found worldwide and is found in the saliva of the majority of adults (>90%). It infects almost all children by the age of two and the infection is life-long. Again, it replicates in B and T lymphocytes, megakaryocytes, glioblastoma cell and in the oropharynx. It can set up a latent infection in T cells which can later be activated when the cells are stimulated to divide. Infected cells are larger than normal with inclusions in both cytoplasm and nucleus. Cell-mediated immunity is essential in control, although infection is life-long, and the virus can reactivate in immune-suppression. The receptor for this virus is not known.
Pathogenesis
Human herpes virus-6 has two forms, HHV-6A and HHV-6B. The latter causes exanthem
subitum, otherwise known as roseola infantum. This a common disease of young children (in the US >45% of children
are seropositive for HHV-6 by two years of age) and symptoms include fever and sometimes
upper respiratory tract infection and lymphadenopathy. The symptoms last a few
days after an incubation period of around 14 days. The fever subsides leaving a
macropapular rash on the trunk and neck that last a few days longer. In adults,
primary infection is associated with a mononucleosis. This virus was originally
isolated from patients with a lymphoproliferative disease and may co-infect
HIV-infected T4 lymphocytes exacerbating the replication of HIV. Patients with
HIV have a higher infection rate than the normal population. HHV-6 has
been associated with a number of neurological disorders, including encephalitis and
seizures. It has been postulated to play a role in multiple sclerosis and chronic fatigue immunodeficiency syndrome.
WEB RESOURCES
Human
herpes virus 6
from Expert Reviews in Molecular Medicine
This virus binds to the CD4 antigen and replicates in T4 (CD4+) cells and is found in the saliva of the
majority of the adult population (>75%). Most people acquire the infection as
children and it remains with them for the rest of their lives. It is similar to
HHV-6 and may be responsible for some cases of exanthem subitum
WEB RESOURCES
Human
herpes virus 7
from Expert Reviews in Molecular Medicine
Human herpes virus 8
This was formerly known as Kaposi=s
sarcoma associated herpes virus and is found in the saliva of many AIDS
patients. It infects peripheral blood lymphocytes. The distribution of the virus
may explain why some populations of HIV-infected people go down with Kaposi=s
sarcoma while others do not. For further details see the AIDS/HIV section
Herpes B
This is a simian virus found in old world monkeys such as macaques but it can be a human pathogen in people who handle monkeys (monkey bites are the route of transmission). In humans, the disease is much more problematic than it is in its natural host. Indeed, about 75% of human cases result in death with serious neurological problems (encephalitis) in many survivors. There is also evidence that the disease can be passed from a monkey-infected human to another human. In vitro the virus is sensitive to both Acyclovir and Ganciclovir and these are recommended for therapy. Their efficacy is unknown.
![]() Return to the Virology section of Microbiology and Immunology On-line
Return to the Virology section of Microbiology and Immunology On-line
![]() Return to the Department of Microbiology and Immunology Site Guide
Return to the Department of Microbiology and Immunology Site Guide
This page
copyright 2001, The Board of Trustees of the University of South Carolina
This page last changed on Wednesday, November 28, 2001
Page maintained by Richard Hunt
URL: http://www.med.sc.edu:85/virol/herpes.htm
Please report any problems to rhunt@med.sc.edu