|
x |
x |
|
 |
 |
|
INFECTIOUS
DISEASE |
BACTERIOLOGY |
IMMUNOLOGY |
MYCOLOGY |
PARASITOLOGY |
VIROLOGY |
|
PORTUGUESE |
BACTERIOLOGY - CHAPTER ELEVEN
ENTEROBACTERIACEAE, VIBRIO, CAMPYLOBACTER AND
HELICOBACTER
Dr Alvin Fox
Emeritus Professor
University of South Carolina School of Medicine
|
|
TURKISH |
|
ALBANIAN |
|
SPANISH |
|
SLOVAK |
|
SEARCH |
Let us know what you think
FEEDBACK |
|
|
|

 |
|
Logo image © Jeffrey
Nelson, Rush University, Chicago, Illinois and
The MicrobeLibrary |
|
|
|
KEY WORDS
Opportunistic Gastroenteritis
Diarrhea
Dysentery
Urinary tract
infections
Lactose
positive/negative
API strip
Enteropathogenic
E. coli
Enterotoxigenic
E. coli
Heat stable
toxin
Heat labile
toxin
Enteroinvasive
E. coli
Enterohemorrhagic
E. coli
Vero toxin
(Shiga-like)
Hemolysin
Adhesive
pili
Shigella
Bacillary
dysentery
Shiga toxin
Salmonella
typhi
Typhoid
Vi antigen
Salmonella
enteritidis (salmonellosis)
Salmonella
cholerae-suis
Vibrio
cholerae
Cholera
Choleragen
(cholera toxin)
Yersinia
entercolitica
Campylobacter
jejuni
Helicobacter pylori |
ENTEROBACTERIACEAE
General
This group of organisms includes several that cause
primary infections of the human gastrointestinal tract. Thus, they are referred
to as enterics (regardless of whether they cause gut disorders). Bacteria that
affect the
gastrointestinal tract include certain strains of Escherichia coli and Salmonella,
all 4 species of Shigella, and Yersinia entercolitica. The
rheumatic disease, Reiter's syndrome (associated with HLA-B27), can result from
prior exposure to Salmonella, Shigella, or Yersinia. Other
organisms that are not members of the Enterobacteriacae, including
Campylobacter and Chlamydia, are also causative agents of Reiter's
syndrome. Yersina pestis (the cause of "plague") will be
considered separately with other
zoonotic organisms.
Members of this family are major causes of
opportunistic infection (including septicemia, pneumonia, meningitis and urinary
tract infections). Examples of genera that cause opportunistic infections are:
Citrobacter, Enterobacter, Escherichia, Hafnia, Morganella,
Providencia and Serratia. Selection of antibiotic therapy
is complex due to the diversity of organisms.
Some of the organisms additionally cause community-acquired
disease in otherwise healthy people. Klebsiella pneumoniae is often
involved in respiratory infections. The organism has a prominent capsule aiding
pathogenicity . The commonest community acquired ("ascending") urinary
tract infection is caused by E. coli. The vast majority of urinary tract
infections are ascending, often from fecal contamination. Proteus is
another common cause of urinary tract infection; the organism produces a
urease
that degrades urea producing an alkaline urine.
Isolation and identification of
Enterobacteriaceae
Enterobacteriaceae are Gram-negative facultative anerobic rods.
They lack cytochrome oxidase and are referred to as oxidase-negative. They are
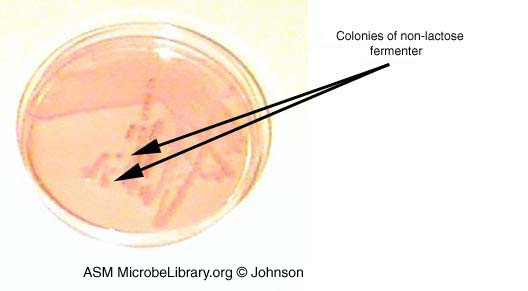
often isolated from fecal matter on agar containing lactose and a pH indicator.
Colonies that ferment lactose will produce sufficient acid to cause a color
shift in the indicator (Figure 1). Escherichia coli is a fermenter of lactose, while Shigella,
Salmonella and Yersinia are non-fermenters.
"Non-pathogenic" strains of E. coli (and other lactose-positive
enterics) are often present in normal feces. Since they are difficult to
differentiate from "pathogenic" E. coli, lactose-negative
colonies are often the only ones identified in feces. All Enterobacteriaceae
isolated from other sites (which contain low numbers of bacteria (e.g. urine) or
are normally sterile (e.g. blood)) are identified biochemically, for example
using the API 20E
system. Important serotypes can be differentiated by their O (lipopolysaccharide),
H (flagellar) and K (capsular) antigens. However,
serotyping is generally not
performed in the routine clinical laboratory.
|
 Figure 1A Reactions in TSI agar slants.
For more information on this figure, please go
here.
© Neal R. Chamberlain, Kirksville College of Osteopathic Medicine, Kirksville, MO
and
The MicrobeLibrary
Figure 1A Reactions in TSI agar slants.
For more information on this figure, please go
here.
© Neal R. Chamberlain, Kirksville College of Osteopathic Medicine, Kirksville, MO
and
The MicrobeLibrary
|
 Figure 1B Nonlactose fermenter on Hektoen agar which contains
bile salts and acid indicators (bromthymol blue and acid fuchsin). The
gram-positive bacteria are inhibited so the agar is selective for gram-negative
bacteria. The lactose fermenters form orange colonies while the nonfermenters
appear green to blue-green. This is especially helpful in distinguishing
potential pathogens from normal flora in stool specimens. However, it is
difficult to tell the non-fermenters from each other. The organism on this plate
could be Salmonella, Proteus, or Shigella. © Pat Johnson,
Palm Beach Community College, Lake Worth, Florida
and
The MicrobeLibrary
Figure 1B Nonlactose fermenter on Hektoen agar which contains
bile salts and acid indicators (bromthymol blue and acid fuchsin). The
gram-positive bacteria are inhibited so the agar is selective for gram-negative
bacteria. The lactose fermenters form orange colonies while the nonfermenters
appear green to blue-green. This is especially helpful in distinguishing
potential pathogens from normal flora in stool specimens. However, it is
difficult to tell the non-fermenters from each other. The organism on this plate
could be Salmonella, Proteus, or Shigella. © Pat Johnson,
Palm Beach Community College, Lake Worth, Florida
and
The MicrobeLibrary
 Figure 1B Growth of a nonlactose fermenter
on MacConkey agar which contains bile salts and crystal violet which inhibit the
growth of gram-positive bacteria. The agar also contains lactose and a red dye
that differentiates the lactose fermenters from the non-fermenters. Colonies of
lactose fermenting bacteria are pink to red while the nonfermenters are
colorless or transparent. This agar does not distinguish between the non-lactose
fermenters; this growth could indicate several organisms - Proteus, Salmonella
or Shigella, for example. In a stool specimen, it would be enough
evidence to continue with further identification. © Pat Johnson, Palm Beach
Community College, Lake Worth, Florida
and The MicrobeLibrary
Figure 1B Growth of a nonlactose fermenter
on MacConkey agar which contains bile salts and crystal violet which inhibit the
growth of gram-positive bacteria. The agar also contains lactose and a red dye
that differentiates the lactose fermenters from the non-fermenters. Colonies of
lactose fermenting bacteria are pink to red while the nonfermenters are
colorless or transparent. This agar does not distinguish between the non-lactose
fermenters; this growth could indicate several organisms - Proteus, Salmonella
or Shigella, for example. In a stool specimen, it would be enough
evidence to continue with further identification. © Pat Johnson, Palm Beach
Community College, Lake Worth, Florida
and The MicrobeLibrary
 Figure 1C Growth of gram-negative bacteria that cannot
ferment lactose on eosin methylene blue (EMB) agar which contains bile salts and
dyes which inhibit growth of gram-positive bacteria. Growth on EMB agar is a
useful diagnostic tool to distinguish between lactose fermenters and non-fermenters
which will appear colorless. Salmonella and Shigella, both
non-lactose fermenting pathogens, can be distinguished from the more common
intestinal flora which ferment lactose.
© Pat Johnson, Palm Beach Community College, Lake Worth, Florida
and
The MicrobeLibrary
Figure 1C Growth of gram-negative bacteria that cannot
ferment lactose on eosin methylene blue (EMB) agar which contains bile salts and
dyes which inhibit growth of gram-positive bacteria. Growth on EMB agar is a
useful diagnostic tool to distinguish between lactose fermenters and non-fermenters
which will appear colorless. Salmonella and Shigella, both
non-lactose fermenting pathogens, can be distinguished from the more common
intestinal flora which ferment lactose.
© Pat Johnson, Palm Beach Community College, Lake Worth, Florida
and
The MicrobeLibrary
|
|
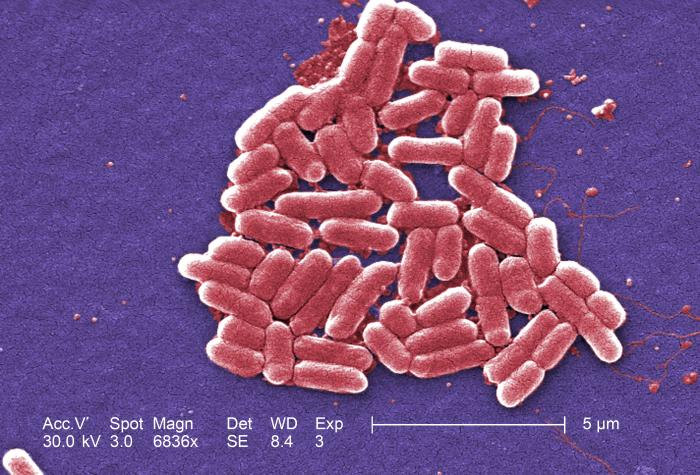
 Figure 2
Figure 2
Colorized scanning electron micrograph. Gram-negative Escherichia coli
bacteria of the strain O157:H7 6836x. CDC
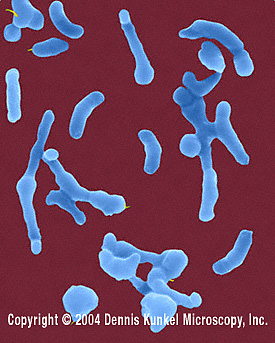
 Figure 3 E. coli (0157:H7) hemorrhagic type. Gram-negative,
enteric, facultatively anaerobic, rod prokaryote. Potentially fatal to
humans, contracted when contaminated meat is cooked inadequately. ©
Dennis Kunkel Microscopy, Inc.
Used with permission
Figure 3 E. coli (0157:H7) hemorrhagic type. Gram-negative,
enteric, facultatively anaerobic, rod prokaryote. Potentially fatal to
humans, contracted when contaminated meat is cooked inadequately. ©
Dennis Kunkel Microscopy, Inc.
Used with permission |
Gastroenteritis, diarrhea and dysentery
Escherichia
coli
E. coli (figure 3) live in the human gut and are usually harmless but some
are pathogenic causing diarrhea and other symptoms as a result of ingestion
of contaminated food or water.
At the species level, E. coli and Shigella
are indistinguishable. For practical reasons (primarily to avoid confusion), they
are not placed in the same genus. Not surprisingly there is a lot of overlap
between diseases caused by the two organisms.
1) Enteropathogenic E. coli (EPEC). Certain
serotypes are commonly found associated with infant diarrhea. The use of gene
probes has confirmed these strains as different from other groups listed below.
There is a characteristic morphological lesion with destruction of microvilli
without invasion of the organism which suggests adhesion is important.
Clinically, one observes:
- fever
- diarrhea
- vomiting
- nausea usually with
non-bloody stools
2) Enterotoxigenic E. coli (ETEC) produce
diarrhea resembling cholera but much milder in degree. They also cause "travelers'
diarrhea". Two types of plasmid-encoded toxins are produced.
- Heat labile
toxins which are similar to choleragen (see cholera section below). Adenyl
cyclase is activated with production of cyclic AMP and increased secretion of
water and ions.
- Heat stable toxins. Guanylate cyclase is activated which
inhibits ionic uptake from the gut lumen. Watery diarrhea, fever and nausea
result in both cases.
3) Enteroinvasive E. coli (EIEC ) produce a
dysentery (indistinguishable clinically from shigellosis, see bacillary
dysentery below).
4) Enterohemorrhagic E. coli (EHEC). These
are usually serotype O157:H7 (figure 2, 3, 4a). Other kinds of EHEC are sometimes called
"non-O157 EHEC". E. coli serogroups
O26, O111, and O103 are those that most often
cause illness in people in the United States.
Most non-O157 EHECs cause less severe disease
than O157:H7 but a few can cause more severe
symptoms. Very often, non-O157 EHECs are not
identified and much less is known about them.
|
 Figure 4A Transmission electron micrograph of Escherichia coli O157:H7
CDC/Peggy S. Hayes
psh1@cdc.gov
Figure 4A Transmission electron micrograph of Escherichia coli O157:H7
CDC/Peggy S. Hayes
psh1@cdc.gov
 Figure 4B Chronology of E. coli O157:H7 infections, an emerging type of foodborne illness.
CDC
Figure 4B Chronology of E. coli O157:H7 infections, an emerging type of foodborne illness.
CDC
|
These organisms can produce a hemorrhagic colitis
(characterized by bloody and copious diarrhea with few leukocytes in
afebrile
patients). However, they are taking on increasing importance (figure 4b) with the recognition
of outbreaks caused by contaminated hamburger meat. The organisms can
disseminate into the bloodstream producing systemic hemolytic-uremic syndrome
(hemolytic anemia, thrombocytopenia and kidney failure) which is often fatal.
Around 5–10% of those who are diagnosed with EHEC infection develop a
potentially life-threatening hemolytic uremic syndrome.
Production of Vero
toxin (biochemically similar to Shiga toxin - thus also known as "Shiga-like")
is highly associated with this group of organisms. The toxin is encoded by a lysogenic phage.
Hemolysins (plasmid-encoded) are also important in pathogenesis.
Since these bacteria make Shiga-like toxins, they are often called
“Shiga toxin-producing” E. coli, or STEC for short. They are
also called Verocytotoxic E. coli (VTEC); these all refer to
the same group of bacteria.
As noted above, there are at least four etiologically
distinct diseases. However, in the diagnostic laboratory, the groups
are not generally differentiated and treatment is based on symptomatology.
Usually, fluid
replacement is the primary treatment. Antibiotics are generally not used except
in severe disease or disease that has progressed to a systemic stage (e.g. hemolytic-uremia
syndrome).
Two major classes of pili are produced by E.
coli: mannose-sensitive and mannose-resistant pili. The former bind to
mannose containing glyocoproteins and the latter to cerebrosides on the host
epithelium, allowing attachment. This aids in colonization by E. coli.
|
 Figure 5. Shigella dysenteriae - Gram-negative, enteric,
facultatively anaerobic, rod prokaryote; causes bacterial dysentery. This
species is most often found in water contaminated with human feces. ©
Dennis Kunkel Microscopy, Inc.
Used with permission
Figure 5. Shigella dysenteriae - Gram-negative, enteric,
facultatively anaerobic, rod prokaryote; causes bacterial dysentery. This
species is most often found in water contaminated with human feces. ©
Dennis Kunkel Microscopy, Inc.
Used with permission |
Shigella
There are about 14,000 reported cases of
shigellosis in the United States each year
but because many milder cases are not
diagnosed, the actual number of infections
is thought to be at least twenty times
greater. Shigellosis is particularly common
and causes recurrent problems in settings
with poor hygiene where epidemics can occur.
It is diagnosed more often in summer than
winter with children between the ages of 2
to 4 years being the most prone to
infection. Often the disease is seen in
child care facilities and many cases are the
result of the spread of the illness in
families with small children. Shigella
pass from an infected person to another as
they are present in the diarrheal stools.
Stools can be infectious while the patient
is sick and for up to two weeks after. Most
Shigella infections are the result
of the bacterium passing from stools or
soiled fingers of one person to the mouth of
another person. Thus, hygiene is important
in containing an outbreak. In the
developing world, shigellosis is far more
common and is present in most communities
most of the time.
Shigella (4
species; S. flexneri, S. boydii, S. sonnei, S.
dysenteriae (figure 5)) all cause bacillary dysentery or shigellosis, (bloody feces
associated with intestinal pain). The organism invades the epithelial lining
layer but does not penetrate. Usually within 2 to 3 days, dysentery results from
bacteria damaging the epithelial layers lining the intestine, often with
release of mucus and blood (found in the feces) and attraction of leukocytes
(also found in the feces as "pus"). However, watery
diarrhea is frequently observed with no evidence of dysentery. Shiga toxin (chromosomally-encoded), which is
neurotoxic,
enterotoxic and
cytotoxic, plays a role. Its
enterotoxicity can make the disease clinically appear as a diarrhea. The toxin
inhibits protein synthesis (acting on the 70S ribosome and lysing 28S rRNA).
This is primarily a disease of young children occurring by fecal-oral contact.
Adults can catch this disease from children, although it can be transmitted by
infected adult food handlers who contaminate food. The source in each case is
unwashed hands. Man is the only "reservoir".
Managing of dehydration is of primary concern.
Indeed, mild diarrhea is often not recognized as shigellosis. Patients with
severe dysentery are usually treated with antibiotics (e.g. ampicillin). In
contrast to salmonellosis, patients respond to antibiotic therapy and disease
duration is diminished.
|
 Figure 6a. Salmonella - rod prokaryote (dividing); note the flagella. Causes salmonellosis (food poisoning).
(x 20,800) ©
Dennis Kunkel Microscopy, Inc.
Used with permission
Figure 6a. Salmonella - rod prokaryote (dividing); note the flagella. Causes salmonellosis (food poisoning).
(x 20,800) ©
Dennis Kunkel Microscopy, Inc.
Used with permission
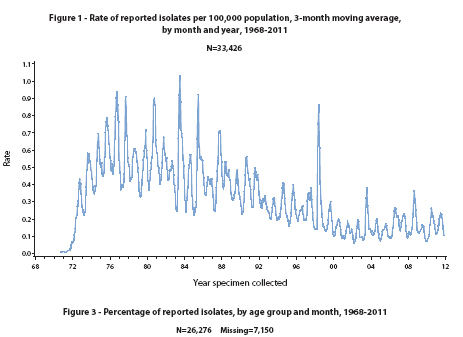
 Figure 6b
Figure 6b
Rate of reported Salmonella isolates in US per
100,000 population, 3-month moving average by month and year 1968-2011
CDC
 Figure 7a
Figure 7a
Computer-generated image of five drug-resistant Salmonella serotype
Typhi bacteria based upon scanning electron micrographic image. Note
the presence of numerous thin, short fimbriae emanating from the organisms’
cell wall, imparting a furry appearance to these bacteria, and the multiple
peritrichous flagella.
CDC/Melissa Brower
 Figure 7b
Figure 7b
Rose spots on the chest of a patient with typhoid fever due to the bacterium
Salmonella typhi.
CDC/ Armed Forces Institute of Pathology, Charles N. Farmer |
Salmonella
It is estimated that Salmonella cause more than 1.2 million
illnesses each year in the United States, resulting in more than 23,000
hospitalizations and 450 deaths. The overall rate of Salmonellosis is
falling in the United States although outbreaks periodically occur (figure
6b).
Salmonella infections most often cause vomiting or diarrhea,
sometimes severe. In rare cases, Salmonella illness can lead to severe and
life-threatening bloodstream infections.
Based on genetic studies, there is a single species
of Salmonella (Salmonella enterica) (figure 6a). At the other extreme using
appropriate antibodies, more than 2000 antigenic "types" have been
recognized. There are, however, only a few types that are commonly associated
with characteristic human diseases (most simply referred to as Salmonella enteritidis,
Salmonella cholerae-suis and Salmonella typhi).
Salmonellosis
Salmonellosis, the common salmonella infection, is
caused by a variety of serotypes (most commonly S. enteritidis) and
is transmitted from contaminated food (such as poultry and eggs). It does not
have a human reservoir and usually presents as a gastroenteritis (nausea,
vomiting and non-bloody stools). The disease is usually self-limiting (2 - 5
days). Like Shigella, these organisms invade the epithelium and do not produce
systemic infection. In uncomplicated cases of salmonellosis, which are the vast
majority, antibiotic therapy is not useful. S. cholerae-suis (seen much
less commonly) causes septicemia after invasion. In this case, antibiotic
therapy is required.
Typhoid
The severest form of salmonella infections,
"typhoid" (enteric fever), caused by Salmonella typhi (figure 7a),
is
not often seen in the United States, although it is one of the historical causes of widespread
epidemics and still is in the third world. It is estimated that about 5,700
cases occur annually in the United States. Most cases (up to 75%) are
acquired while traveling internationally. Typhoid fever affects about 21.5
million persons each year in the developing world.
The organism is transmitted from a
human reservoir or in the water supply (if sanitary conditions are poor) or in
contaminated food. It initially invades the intestinal epithelium and, during
this acute phase, gastrointestinal symptoms are noted. The organisms penetrates
(usually within the first week) and passes into the bloodstream where it is
disseminated in macrophages. Symptoms of typhoid include a fever up to
103° to 104° F (39° to 40° C). The patient may also feel weak and have
stomach pains, headache, and/or loss of appetite. In some cases, patients
have a rash of flat, rose-colored spots (figure 7b). Diagnosis of typhoid
fever is carried out from stool or blood samples that are tested for the
presence of Salmonella typhi.
Typical features of a systemic bacterial infection
are seen. The septicemia usually is temporary with the organism finally lodging
in the gall bladder. Organisms are shed into the intestine for some weeks. At
this time, gastroenteritis (including diarrhea) is noted again. The Vi
(capsular) antigen plays a role in the pathogenesis of typhoid. A carrier state
is common; thus one person (e.g. a food handler) can cause a lot of spread.
Antibiotic therapy is essential. Unfortunately, there is increasing
resistance to antibiotics, including fluoroquinolones and, as a result there
may be increases in case-fatality rates. Epidemics and high endemic disease
rates occur in the Central Asian Republics, the Indian subcontinent, and
across Asia and the Pacific Islands.
Most people in the United States are not vaccinated against typhoid but
those traveling to a country where typhoid is common, should consider being
vaccinated against typhoid. There are two vaccines available: Ty21a, taken
orally in a capsule and ViCPS, taken by injection. Both need boosters after a
number of years.
|
 Figure 7c
Figure 7c
Yersinia enterocolitica - Gram-negative, facultatively anaerobic, rod
prokaryote (dividing). This bacterium releases a toxin that causes enteritis
with pain resembling appendicitis.
©
Dennis Kunkel Microscopy, Inc.
Used with permission |
Yersinia entercolitica
Yersinia entercolitica (figure 7c)
infection (Yersiniosis)
is a major cause of gastroenteritis (the main clinical symptom) in Scandinavia
and elsewhere and is seen in the United States. The organisms are invasive (usually without
systemic spread). Typically the infection is characterized by diarrhea, fever and abdominal pain.
Y. enterocolitica infections are seen most often in young children
in whom symptoms include:
- fever
- abdominal pain
- diarrhea, which is often bloody.
These symptoms usually develop 4 to 7 days after infection and can last
for one to three weeks or more. In older children and adults predominant
symptoms include:
- right-sided abdominal pain (this may lead to confusion with
appendicitis)
- fever
In a few cases, complications including skin rash, joint pains, or
bacteremia
can occur.
Uncomplicated cases of diarrhea due to Y.
enterocolitica usually resolve without
antibiotics but in more severe or complicated
infections the use of antibiotics such as
aminoglycosides, doxycycline,
trimethoprim-sulfamethoxazole, or fluoroquinolones
is recommended.
Y. enterocolitica can be
transmitted by fecal contamination of water or milk by domestic animals or from
eating meat products. It is best isolated by "cold" enrichment: when
refrigerated this organism survives while others do not.
Yersinia pseudotuberculosis
A similar, but less
severe, disease is caused by Y. pseudotuberculosis. The disease is
characterized by
Secondary symptoms include
Outbreaks have been reported in Canada,
Japan, Finland and Russia (among others). Only in a few of the outbreaks has
the vector or source of the infection been identified. Unwashed vegetables
including iceberg lettuce and carrots have been implicated by epidemiologic
investigations as a source of infection; however, the source of the
contamination has not been identified.
|
|
|
Vibrio species
Several species of vibrio are known to cause human
disease and there are an estimated 80,000 illnesses,
500 hospitalizations and 100 deaths each year in the
United States.
Vibrio
cholerae
These are Gram-negative rods. They are
comma shaped,
facultative anaerobes which are oxidase positive. The most important vibrio, Vibrio
cholerae (figure 8), is the causative agent of cholera. It has simple nutritional
requirements and is readily cultivated. V. cholerae is found in the feces
of an infected individual and ends up in the water supply if sewage is
untreated. The organism is thus transmitted by drinking contaminated water. The
organism survives in fresh water and, like other vibrios, in salt water. Food,
after water contamination, is another means of transmission. Thus, it is
primarily a disease of the third world. In the United States, it is observed in the
occasional international traveler (especially to parts of Africa, Southeast Asia,
or Haiti), although it is sometimes seen after ingestion of seafood.
Once in the gut, the organism adheres to the epithelium of the intestine without
penetration. Adhesion to the microvilli is thus important in pathogenesis.
Cholera toxin is then secreted.
Choleragen (cholera toxin) is
chromosomally encoded and contains two types of subunit (A and B). The B subunit
binds to gangliosides on epithelial cell surfaces allowing internalization of
the A subunit. B subunits may provide a hydrophobic channel through which A
penetrates. The A subunit catalyses ADP-ribosylation of a regulator complex
which in turn activates adenylate cyclase present in the cell membrane of the
epithelium of the gut. The overproduction of cyclic AMP in turn stimulates
massive secretion of ions and water into the lumen. Dehydration and death
(without treatment) result. Thus, fluid replacement is the major component of
treatment. Antibiotic therapy (including tetracycline) is additionally used. Vaccination is only partially effective and not generally recommended.
It is most commonly used by international travelers.
Cholera is usually an acute,
diarrheal illness. It is often mild or asymptomatic, but sometimes it
can be more severe. About 5-10% of infected patients develop severe cholera, the
early symptoms of which include (CDC):
-
profuse watery diarrhea,
sometimes described as “rice-water stools,”
-
vomiting
-
rapid heart rate
-
loss of skin elasticity
-
dry mucous membranes
-
low blood pressure
-
thirst
-
muscle cramps
-
restlessness or irritability
This can lead to:
If untreated, severe dehydration
can rapidly lead to shock and death.
As noted above, diarrhea from
people with cholera contains large amounts of infectious bacteria that
can contaminate the environment (such as water supplies or food) and
infect others, if ingested, thereby spreading the disease. Improved
sanitary conditions can prevent the spread of cholera. Washing hands
after touching anything that might be contaminated and properly
disposing of contaminated items and human waste is essential.
In severe cases of cholera, CDC recommends:
-
Oral or intravenous hydration is the mainstay
of cholera treatment
-
In conjunction with hydration, treatment with
antibiotics is recommended for severely ill patients. It is
particularly recommended for patients who are severely or moderately
dehydrated and continue to pass a large volume of stool during
rehydration treatment. Antibiotic treatment is also recommended for
all patients who are hospitalized.
-
Antibiotic choices should be informed by local
antibiotic susceptibility patterns. In most countries, Doxycycline
is recommended as first-line treatment for adults, while
azithromycin is recommended as first-line treatment for children and
pregnant women. During an epidemic or outbreak, antibiotic
susceptibility should be monitored through regular testing of sample
isolates from various geographic areas.
-
None of the guidelines recommend antibiotics as
prophylaxis for cholera prevention, and all emphasize that
antibiotics should be used in conjunction with aggressive hydration.
-
Education of health care workers, assurance of
adequate supplies, and monitoring of practices are all important for
appropriate dispensation of antibiotics.
Vibrio parahemolyticus
Vibrio parahemolyticus (figure 9) is the agent that causes vibriosis and
is usually transmitted by ingestion of raw seafood (especially oysters).
An estimated 4,500 cases of vibriosis occur each year in the United
States. The organism lives in brackish saltwater and causes
gastrointestinal illness in humans.
Vibrio parahemolyticus inhabits coastal waters in the United
States and Canada and is present in higher concentrations during summer;
it grows best in high concentrations of salt (i.e. it is halophilic). A non-bloody
diarrhea is observed but it is not as severe as cholera.
There was an increase in Vibrio parahaemolyticus
illnesses associated with consumption of shellfish from several Atlantic
coast harvest areas in the United States in 2013 (figure 9).
The symptoms of vibriosis are (CDC):
Usually these symptoms occur within 24 hours of
ingestion of the bacterium. The disease is usually self-limiting and
lasts 3 days. Severe disease is rare and occurs more commonly in persons
with weakened immune systems. V. parahaemolyticus can also
cause an infection of the skin when an open wound is exposed to warm
seawater.
Diagnosis is by isolation of the bacterium from cultures
of stool, wound, or blood. For isolation from stool, the use of a
selective medium that has thiosulfate, citrate, bile salts, and sucrose
(TCBS agar) is recommended by CDC.
Usually treatment is not necessary and there is no
evidence that antibiotic treatment decreases the severity or the length
of the illness. The patient should be encouraged to drink plenty of
water to replace fluids lost through diarrhea. In severe or prolonged
illnesses, antibiotics such as tetracycline or ciprofloxicin can be
used.
Vibrio vulnificus
Vibrio vulnificus (figure 9d) is another salt
loving (halophilic) bacterium that causes cases of vibriosis and again
disease is caused by eating contaminated raw seafood or exposure of an
open wound to contaminated sea water. In the latter case, infection can
lead to skin breakdown and ulceration. Between 1988 and 2006, CDC
received reports of more than nine hundred V. vulnificus
infections from the Gulf Coast states, where most cases occur.
Infection by V. vulnificus can cause, in
non-immunocompromised people:
-
vomiting
-
diarrhea
-
abdominal pain
In immunocompromised people, especially those with
chronic liver disease, V. vulnificus can infect the bloodstream (bacteremia),
resulting in a severe disease that can be life-threatening. It is
characterized by:
About half of V. vulnificus bloodstream
infections result in death.
Diagnosis is by stool, wound, or blood cultures.
If V. vulnificus is suspected, treatment should
be initiated immediately because antibiotics improve survival with
aggressive treatment of the wound site; debridement of infected necrotic
tissue or amputation of the infected limb is sometimes necessary.
Doxycycline and cephalosporin are indicated or a fluoroquinolone such as
levofloxacin, ciprofloxacin or gatifloxacin. Children, in whom
doxycycline and fluoroquinolones are contraindicated, can be treated
with trimethoprim-sulfamethoxazole plus an aminoglycoside.
|
|
ANIMATION
Pathology of Cholera
© Alan House and Mike Hyman, Department of Microbiology, North Carolina State University, Raleigh, N.C.
and
The MicrobeLibrary
|
|
|
 Figure 8a
Figure 8a
Vibrio cholerae. Leifson flagella stain (digitally colorized).
CDC/Dr. William A. Clark
 Figure 8b
Figure 8b
Vibrio cholerae - Gram-negative, facultatively
anaerobic, curved (vibrio-shaped), rod prokaryote; causes Asiatic cholera. ©
Dennis Kunkel Microscopy, Inc.
Used with permission
 Figure 9a
Figure 9a
Vibrio parahaemolyticus - halophilic, facultative anerobic,
rod bacterium that causes a food-borne illness known as seafood poisoning.
Usually transmitted through eating raw or undercooked seafood such as
oysters. Less commonly, this organism can cause an infection in the skin
when an open wound is exposed to warm seawater.
©
Dennis Kunkel Microscopy, Inc.
Used with permission
 Figure 9b
Figure 9b
Vibrio parahaemolyticus - halophilic, facultative anerobic,
rod bacterium that causes a food-borne illness known as seafood poisoning.
Usually transmitted through eating raw or undercooked seafood such as
oysters. Less commonly, this organism can cause an infection in the skin
when an open wound is exposed to warm seawater.
©
Dennis Kunkel Microscopy, Inc.
Used with permission
 Figure 9c
Figure 9c
Increase in Vibrio parahaemolyticus illnesses associated with
consumption of shellfish from several Atlantic coast harvest areas, United
States, 2013
 Figure 9d
Figure 9d
Scanning electron micrograph of Vibrio vulnificus bacteria; Mag.
13184x CDC
|
 Figure 10a. Campylobacter fetus. Leifson flagella stain (digitally colorized).
CDC/Dr. William A. Clark
Figure 10a. Campylobacter fetus. Leifson flagella stain (digitally colorized).
CDC/Dr. William A. Clark
 Figure 10b
Figure 10b
Campylobacter jejuni is an enteric, curved-rod
prokaryote (bacterium). It is the bacterium that causes campylobacteriosis,
one of the most common bacterial causes of diarrheal illness in the United
States. It is a relatively fragile bacterium that is easily killed by cold
or hot temperatures. Birds are carriers due to their body temperature
being just right to host the bacteria. Improper handling of raw poultry or
undercooked fowl is usually the source of infection in humans. ©
Dennis Kunkel Microscopy, Inc.
Used with permission |
Campylobacter and
Helicobacter
These two groups of Gram-negative
organisms are both curved or spiral shaped and are genetically related.
Campylobacter jejuni
Campylobacteriosis is one of the commonest bacterial
disease causing diarrhea in the United States. There are approximately
14 cases each year per 100,000 population. However, many cases are not
diagnosed and it is estimated that there are over 1.3 million cases
annually. Infections occur much more frequently in the summer than in
winter and the disease occurs in infants and young adults more often
than in older people. It is more often seen in males than females.
Campylobacteriosis is rarely fatal but there are approximately 76 deaths
in the United States among persons with Campylobacter
infections each year.
The most common of the Campylobacter
(figure 10) causing human disease are C. jejuni. The organism infects the
intestinal tract of several animal species (including cattle and sheep) and is a
major cause of cause of abortions. It is transmitted to man in milk
and meat products. Watery diarrhea predominates but dysentery is common. The
organism is invasive but generally less so than Shigella. Malaise, fever
and abdominal pain are other disease features. Bacteremia is observed in a small
minority of cases.
Campylobacter infection is
diagnosed when a culture of a stool
specimen yields the bacterium.
The organism is
microaerophilic and grows best at 42oC.
It is frequently isolated under these conditions using selective media .
It can
be treated with antibiotics but is usually a self-limiting disease.
Patients should drink extra fluids as
long as the diarrhea lasts. Antibiotics
are only used to treat patients with
severe disease or those at high risk for
severe disease. These include patients
with immune systems severely weakened
from medications or other illnesses.
Azithromycin and fluoroquinolones (e.g.,
ciprofloxacin) are commonly used for
treatment of these infections, but
resistance to fluoroquinolones is
common.
Campylobacteriosis can sometimes have
long-term sequelae. These include:
- arthritis.
- Guillain-Barré syndrome. This is
a rare disease that affects the
nerves of the body beginning several
weeks after the diarrheal illness
and results from an attack on body's
nervous system by the immune system
and can result in temporary
paralysis for several weeks. It
requires intensive medical care. It
is estimated that about one in every
1,000 Campylobacter
illnesses leads to Guillain-Barré
syndrome. As many as 40% of
Guillain-Barré syndrome cases in the
United States may result from
campylobacteriosis.
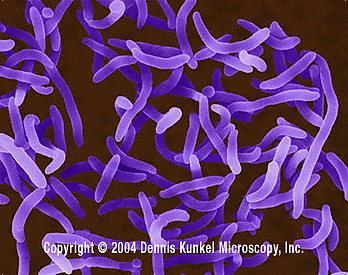
Helicobacter pylori
Helicobacter pylori
(figure
11) has
been accepted in the last few years as the major cause of stomach ulcers. The organism chronically lives in
and on the stomach
mucosa of man. Culture is the preferred method of diagnosis but may miss a
number of cases. The organism characteristically produces a urease which
generates ammonia and carbon dioxide. This aids in detecting and identifying the
isolated organism. Urease is produced in such large amounts that it can be directly
detected in mucosa sampled after endoscopy. Alternatively, 13C or
14C
labeled CO2 is detected in the breath after feeding labeled urea.
Production of ammonia is a factor in pathogenesis (in locally neutralizing
stomach acid). Antibiotic therapy eliminates the organism, peptic ulcers heal
and relapses are generally avoided.
Conclusion
Sanitary measures protect the water
supply, avoiding contamination with sewage. This is the primary reason that
epidemics with life-threatening pathogens (e.g cholera and typhoid) are rarely
seen in western countries but are commonly seen in the third world. Other less severe
diseases (e.g. salmonellosis, EHEC) are still common from eating contaminated
animal products, which has been less well controlled. Shigella, which has
a human host, would be even more difficult to eradicate. Vaccination is rarely
used and, indeed, is an expensive way to go compared to sewage treatment. In
severe diarrhea, fluid replacement is essential. Antibiotic therapy is used in
severe local infection and always in systemic disease.
|
|
|
 Figure 10c
Figure 10c
Campylobacter jejuni - Gram-negative, enteric,
curved (vibrio-shaped), rod prokaryote. Found in the gastrointestinal
tract of humans and animals, it can travel to the oral cavity and
genitourinary tract. Causes gastroenteritis, especially in infants. ©
Dennis Kunkel Microscopy, Inc.
Used with permission
|

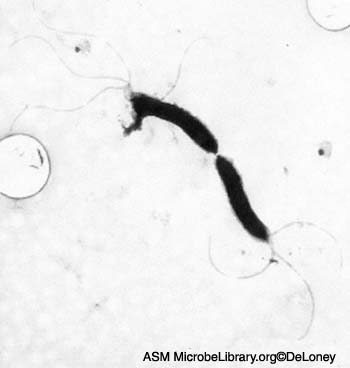
 Figure 11a
Figure 11a
Helicobacter pylori electron micrographs; fastidious microaerophile; typical helical shape shown in EM; causative agent of chronic gastritis, peptic ulcers and gastric cancer. Image can be used to describe the helical morphology of the organism. Average size: 1micron by 2-5 microns. Organism is
in log phase of growth. © Cindy R. DeLoney, Loyola University of Chicago, Chicago, Illinois
and The MicrobeLibrary
 Figure 11b
Figure 11b
Helicobacter pylori - Gram-negative, spiral to pleomorphic, spiral rod
prokaryote. It can move by means of tiny flagella at the end of the cell.
There are many strains of H. pylori which are distinguished by the
human disease with which they cause. H. pylori infection is the main
cause of chronic superficial gastritis and it is associated with both
gastric and duodenal ulcers. It lives in the interface between the surface
of gastric epithelial cells (the lining of the stomach). It often clusters
at the junctions of epithelial cells.
©
Dennis Kunkel Microscopy, Inc.
Used with permission
 Figure 11c
Figure 11c
Helicobacter pylori -
Gram-negative, spiral to pleomorphic, spiral rod prokaryote.
©
Dennis Kunkel Microscopy, Inc.
Used with permission
|
|
|
 Return to the Bacteriology
Section
of Microbiology and Immunology On-line
Return to the Bacteriology
Section
of Microbiology and Immunology On-line
This page last changed on
Monday, February 29, 2016
Page maintained by
Richard Hunt
|