| x | x | |||||||||||||||||||
|
|
 |
|||||||||||||||||||
| BACTERIOLOGY | IMMUNOLOGY | MYCOLOGY | PARASITOLOGY | VIROLOGY | ||||||||||||||||
|
|
|
|||||||||||||||||||
|
Let us know what you think |
||||||||||||||||||||
|
|
||||||||||||||||||||
|
|
||||||||||||||||||||
|
|
||||||||||||||||||||
|
THIS CHAPTER
IS IN SEVERAL PARTS |
||||||||||||||||||||
|
LINKS TO OTHER HIV AND AIDS SECTIONS ARE AT THE BOTTOM OF THIS PAGE |
||||||||||||||||||||
|
WEB RESOURCES Read the original 1981-1982 MMWR reports on a new immunodeficiency disease in the gay community:A Cluster of Kaposi's Sarcoma and Pneumocystis carinii Pneumonia among Homosexual Male Residents of Los Angeles and Orange Counties, California Diffuse, Undifferentiated Non-Hodgkins Lymphoma among Homosexual Males -- United States Important
milestones in the epidemiology of AIDS from CDC. Links to many of the
important MMWR papers
History of AIDS
|
In 1981, clusters of cases of Kaposi's sarcoma (figure 3B) were reported in young patients in San Francisco and New York. This was an unusual occurrence since, in the United States, Kaposi's sarcoma was a rare disease that normally occurs in elderly men of Jewish or Mediterranean ancestry; however, these new clusters of patients were all young male homosexuals and the disease was much more aggressive. Other diseases associated with immunodeficiency also arose in this same homosexual population; particularly of note were Pneumocystis pneumonia (which is an opportunistic infection) and lymphadenopathy (diffuse, undifferentiated non-Hodgkins lymphoma).
Pneumocystis pneumonia, which is caused by a fungal parasite (Pneumocystis carinii - now renamed Pneumocystis jiroveci, figure 3A), was also a very rare disease in the United States. During the period between 1967 and 1978, only five cases of this disease occurred in Los Angeles; however, in 1981 alone, five cases occurred in the same area. Again, all patients were young male homosexuals. The number of sex partners of these patients appeared to be important in that the disease was particularly prevalent among promiscuous individuals and the partners of those individuals. No cases of diffuse, undifferentiated non-Hodgkins lymphoma were reported in the young male (20 to 39 years old) population of the San Francisco area during the period 1977-1980. However, from March 1981 to January 1982, the unusual occurrence of four cases within 10 months was observed; again, these were in the homosexual male population. During 1982, similar immunodeficiencies started to occur in hemophiliacs (July), persons who received blood transfusions (December) and intra-venous drug users who shared needles. Moreover, by January 1983, it was clear that the female sex partners of these patients also got the disease. In view of this, it was obvious that an infectious agent was involved; this agent was either passed during sexual intercourse or by receiving blood (or blood products) from another person. At the same time as these events were occurring in western countries, doctors in Uganda were observing a fatal wasting syndrome that they called slim disease. The patients' cell picture - the selective loss of T4 helper (CD4+) cells - suggests a virus and explains the observed immunodeficiency symptoms. But the causative agent was difficult to identify at first because it does not grow on resting T4 cells. The discovery of HIV depended on the ability to grow the virus in vitro and this required the use of activated T4 cells. The disease was originally termed
Kaposi's Sarcoma and Opportunistic Infections (KSOI) and then Gay-Related Immune Deficiency (GRID) but we now know it as
Acquired
Immuno-Deficiency Syndrome (AIDS or SIDA in French and Spanish). In the
absence of chemotherapy, AIDS is always fatal as a result of immuno-suppression and consequent opportunistic infections.
Worldwide, 60 million people have been infected with HIV and the epidemic has resulted in the deaths of half of AIDS patients.
Currently, there is no vaccine available but, as a result of highly active
anti-retroviral therapy, viral replication can be inhibited and viral load can
be suppressed so that the patient does not progress to AIDS.
The clue to growing HIV came with the realization that, while it did not grow in resting T4 lymphocytes, it would grow on T4 cells that had been activated with a cytokine called interleukin-1 (IL1). The virus was isolated in 1984 by Luc Montanier (Pasteur Institute, Paris), who shared the Nobel Prize for his discovery in 2008, and Robert Gallo (NIH, Bethesda, USA). Montanier called the virus lymphadenopathy virus (LAV) and Gallo, who had discovered the first human leukemia virus (HTLV-1), named the virus HTLV-3. Today we know it as human immunodeficiency virus (HIV). A similar cellular picture is seen in some cases of feline leukemia and HTLV-1 infection, i.e. a selective loss of a specific class of cells giving rise to immune suppression, further suggesting that the cause of AIDS is a virus.
|
|||||||||||||||||||
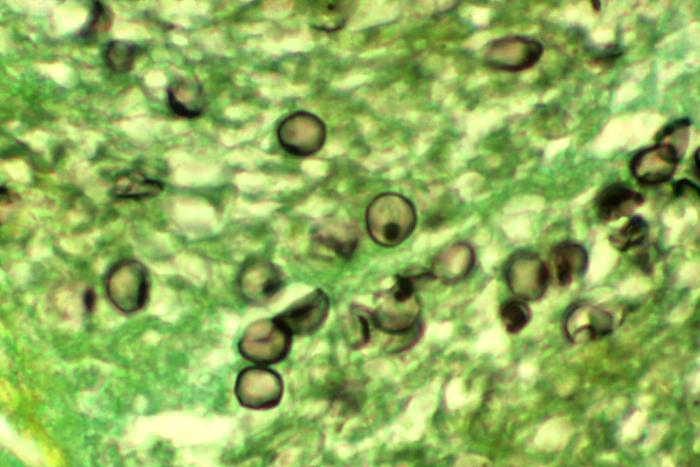 Figure 3A Figure 3ACysts of Pneumocystis carinii in AIDS. Methenamine silver stain. Histopathology of lung shows characteristic cysts with cup forms and dot-like cyst wall thickenings. CDC/ Dr. Edwin P. Ewing, Jr. |
||||||||||||||||||||
|
Figure 3B Kaposi's Sarcoma |
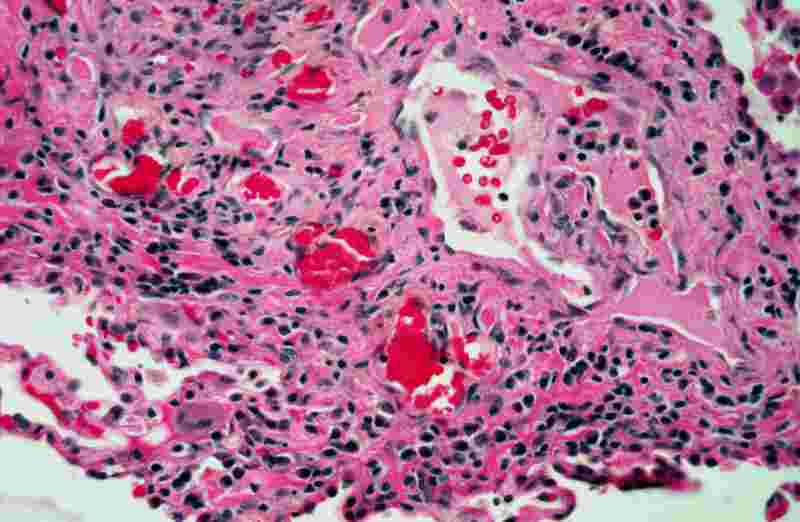 The perivenular infiltrate of Kaposi sarcoma shows a mixture of spindle cells, inflammatory cells, and ectatic vascular spaces.
The Johns Hopkins Autopsy Resource
(JHAR). Image Archive. The perivenular infiltrate of Kaposi sarcoma shows a mixture of spindle cells, inflammatory cells, and ectatic vascular spaces.
The Johns Hopkins Autopsy Resource
(JHAR). Image Archive.
 Skin showing AIDS-associated Kaposi's sarcoma
Bristol
Biomedical Image Archive, University of Bristol. Used with permission Skin showing AIDS-associated Kaposi's sarcoma
Bristol
Biomedical Image Archive, University of Bristol. Used with permission |
|||||||||||||||||||
 Lesions on the
stomach of a patient with Kaposi's sarcoma Lesions on the
stomach of a patient with Kaposi's sarcoma
|
||||||||||||||||||||
|
|
||||||||||||||||||||
|
|
|
|||||||||||||||||||
|
|
|
|||||||||||||||||||